Peer Reviewed
How Would You Diagnose This Red Patch on an Older Man’s Face?
Correct Answer: D. Angiosarcoma
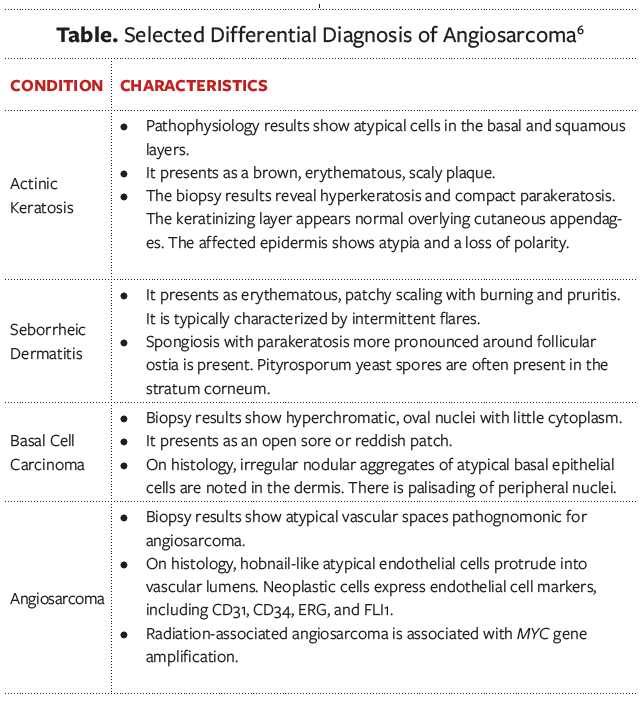
Biopsy results revealed proliferation of atypical vascular spaces, supporting a diagnosis of angiosarcoma.
Persistent facial dermatitis includes a broad differential diagnosis that includes rosacea, seborrheic dermatitis, contact dermatitis, and neoplastic processes (Table). Rosacea can be associated with extensive erythema but is characterized by pustules and papules; lesions are distributed symmetrically around the central face. Seborrheic dermatitis can also lead to extensive erythema with accentuation around the nasolabial folds. There is often pruritus, and scaly patches are characteristic. Lesions from seborrheic dermatitis also involve the face in a symmetrical fashion. Contact dermatitis can be unilateral and is usually associated with itching. Acute lesions are associated with vesicles that are later followed by scaling.

Any progressive lesion that worsens should prompt a biopsy to clarify the diagnosis. Angiosarcoma is rare, but other types of cancer such as lymphoma can be associated with a similar clinical picture. Angiosarcomas may have several different types of presentations.1-3 Lesions may arise in the setting of chronic lymphedema (Stewart-Treves syndrome), in an area previously treated with radiation therapy, or on the head and neck of elderly individuals. A combination of surgical excision, radiotherapy, and angiogenesis inhibitor treatment are helpful. The diffuse nature of most tumors makes complete resection difficult. Paclitaxel is usually the chemotherapeutic agent of choice, with multikinase inhibitors serving as second-line therapeutic agents.2
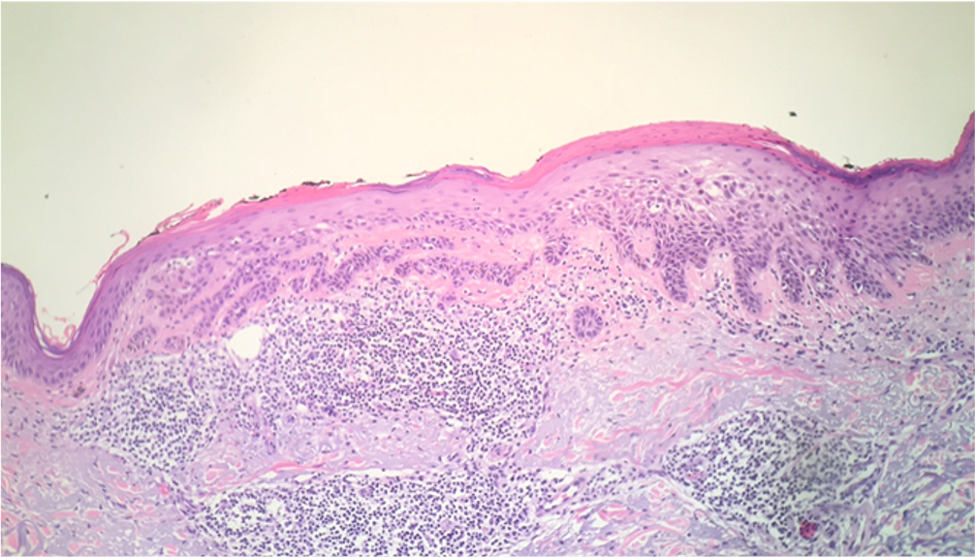
In actinic keratosis, lesions initially appear as small papules or plaques with a sandpaper-like texture. Actinic keratoses are considered premalignant.4 Lesions may turn brown or erythematous and scaly. Histology shows atypical cells in the basal and squamous layers and an absent granular layer along with hyperkeratosis or parakeratosis (Figure 3).5
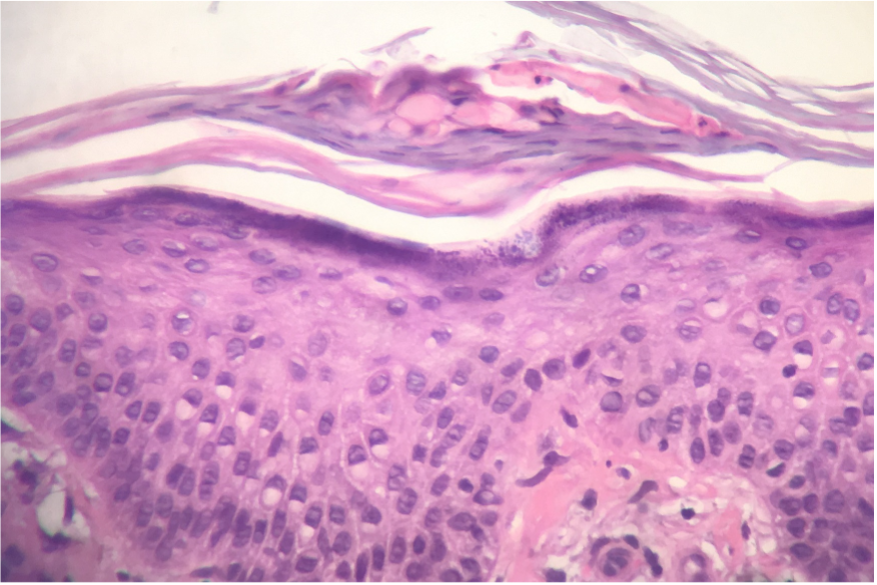
Figure 3. The biopsy would show compact parakeratosis and atypia of the epidermis. Actinic budding would be noted (Hematoxylin and eosin-stained sections; 400× magnification). Image courtesy of Thomas Helm, MD.5Seborrheic dermatitis typically presents in areas of high sebaceous activity. This condition is characterized by intermittent flares with asymptomatic periods and presents as a hyperkeratotic, scaly plaque. Patients exhibit erythematous, patchy scaling associated with burning and pruritis on the face, back, or neck. Histology typically shows spongiosis with parakeratosis around the follicular ostia (Figure 4).
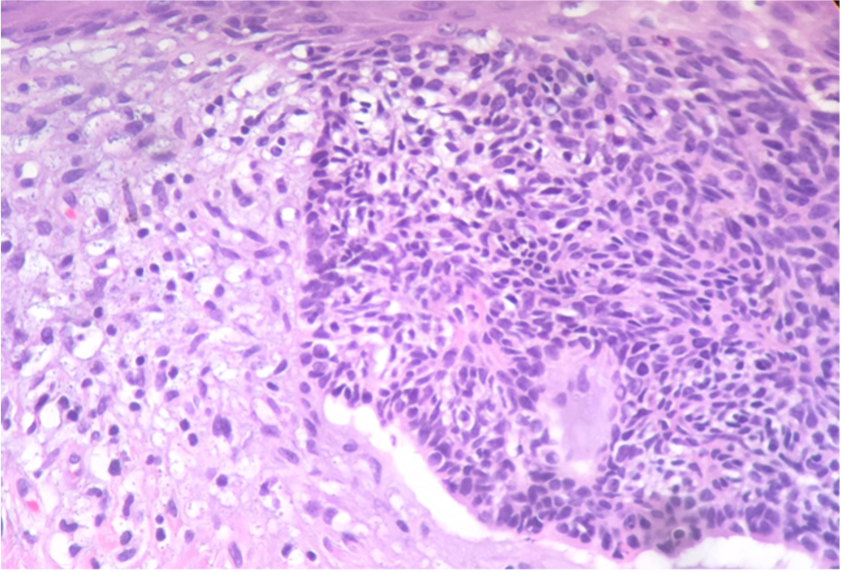
Figure 4. The biopsy would reveal spongiosis and scale crust. Atypia of the epidermis is not identified. (Hematoxylin and eosin-stained sections; 400× magnification) Image courtesy of Thomas Helm, MD.5Basal cell carcinoma typically presents as an open sore, a reddish patch, or a scar-like lesion. The classic presentation location of angiosarcoma is the scalp. Biopsy results in angiosarcoma reveal large, atypical vascular spaces, which do not match up with the typical biopsy presentation of nodular basal cell carcinoma; nodular basal cell carcinoma typically presents with hyperchromatic nuclei and little cytoplasm. Basal cell tumors typically have a peripheral “palisading” pattern of nuclei on histology (Figure 5).
Figure 5. A biopsy would reveal a tumor composed of basaloid cells with scanty cytoplasm. Retraction artifact is noted, and there is peripheral palisading of nuclei (Hematoxylin and eosin-stained sections; 400× magnification). Image courtesy of Thomas Helm, MD.5References
1. Cao J, Wang J, He C, Fang M. Angiosarcoma: a review of diagnosis and current treatment. Am J Cancer Res. 2019;9(11):2303-2313. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6895451/
2. Ishida Y, Otsuka A, Kabashima K. Cutaneous angiosarcoma: update on biology and latest treatment. Curr Opin Oncol. 2018;30(2):107-112. https://doi.org/10.1097/cco.0000000000000427
3. Gupta AK, Bluhm R. Seborrheic dermatitis. J Eur Acad Dermatol Venereol. 2004;18(1):13-20. https://doi.org/10.1111/j.1468-3083.2004.00693.x
4. de Berker D, McGregor JM, Mohd Mustapa MF, Exton LS, Hughes BR. British Association of Dermatologists' guidelines for the care of patients with actinic keratosis 2017. Br J Dermatol. 2017;176(1):20-43. https://doi.org/10.1111/bjd.15107
5. Epithelial neoplasms. In: Clarke LE, Clarke JT, Helm KF. Color Atlas of Differential Diagnosis in Dermatopathology. Jaypee Brothers Medical Publishers Pvt Ltd; 2014;325-346.
6. Malignant dermal neoplasms. Helm KF, Foulke GT, Marks JG Jr. Differential Diagnosis in Dermatology. 2nd ed. JP UK; 2020;299-316.