
Peer Reviewed
An Uncorrected Atrial Septal Defect Presenting as a Rare Cause of Cardiac Cirrhosis
AFFILIATIONS:
1Ascension St. Vincent’s Hospital Indianapolis, Carmel, Indiana
CITATION:
Nallamala H, Cation L. An uncorrected atrial septal defect presenting as a rare cause of cardiac cirrhosis. Consultant. 2023;63(3):e6 doi:10.25270/con.2022.11.000009
Received May 28, 2022. Accepted August 15, 2022. Published online November 30, 2022.
DISCLOSURES:
The authors report no relevant financial relationships.
FUNDING:
This research did not receive grants from any funding agency.
DISCLAIMER:
The authors report that informed patient consent was obtained for publication of the images used herein.
CORRESPONDENCE:
Hinduja Nallamala, DO, 1497 Starcross Lane, Carmel, IN 46280 (hinduja.nallamala@ascension.org)
Introduction. A 66-year-old man presented to the hospital with hypoxia requiring 15 L/min of supplemental oxygen.
Patient history. The patient’s medical history included non-ischemic cardiomyopathy with systolic heart failure, a left ventricular ejection fraction of 30%, and atrial fibrillation.
Diagnostic and laboratory testing. A computed tomography (CT) scan of the patient’s chest with contrast revealed a large right pleural effusion with complete collapse of the right lower lobe, cardiomegaly, and cirrhosis with ascites. A paracentesis revealed a serum-ascites albumin gradient (SAAG) of 1.6 g/dL and an ascitic protein of 3.4 g/dL, which raised concerns for a cardiac etiology of his ascites. A thoracentesis was consistent with a transudative effusion secondary to right-sided heart failure vs hepatic hydrothorax. An echocardiogram with bubble study showed a left ventricular ejection fraction of 30% to 35%, Stage III diastolic dysfunction, left and right atrial dilation, right ventricle enlargement with reduced global right ventricular systolic function, an elevated
![]()
Image 1. Echocardiogram: apical four chamber view shows moderate TR, TR peak gradient of 38 mmHg (reference range <35 mmHg), and TR peak velocity of 309 cm/s (reference range <280 cm/s).
![]()
Image 2. Echocardiogram: apical four chamber view with bubble study shows bubbles in the second ventricular beat.
Portosystemic pressure measurements revealed a hepatic venous pressure gradient (HVPG) of 0 mmHg (normal range), and right hepatic and portal vein pressures within normal limits consistent with a post-hepatic etiology (Figure 1).
![]()
Figure 1. Portal pressures and the etiology of liver cirrhosis.
Thorough imaging and serologic workup for the new onset cirrhosis was negative including a viral hepatitis panel and iron studies. A right heart catheterization revealed sinus venosus ASD with a left to right shunt at the superior vena cava and the right atrium junction. A liver biopsy revealed pericellular fibrosis and sinusoidal dilation confirming cardiac cirrhosis (Images 3 and 4)
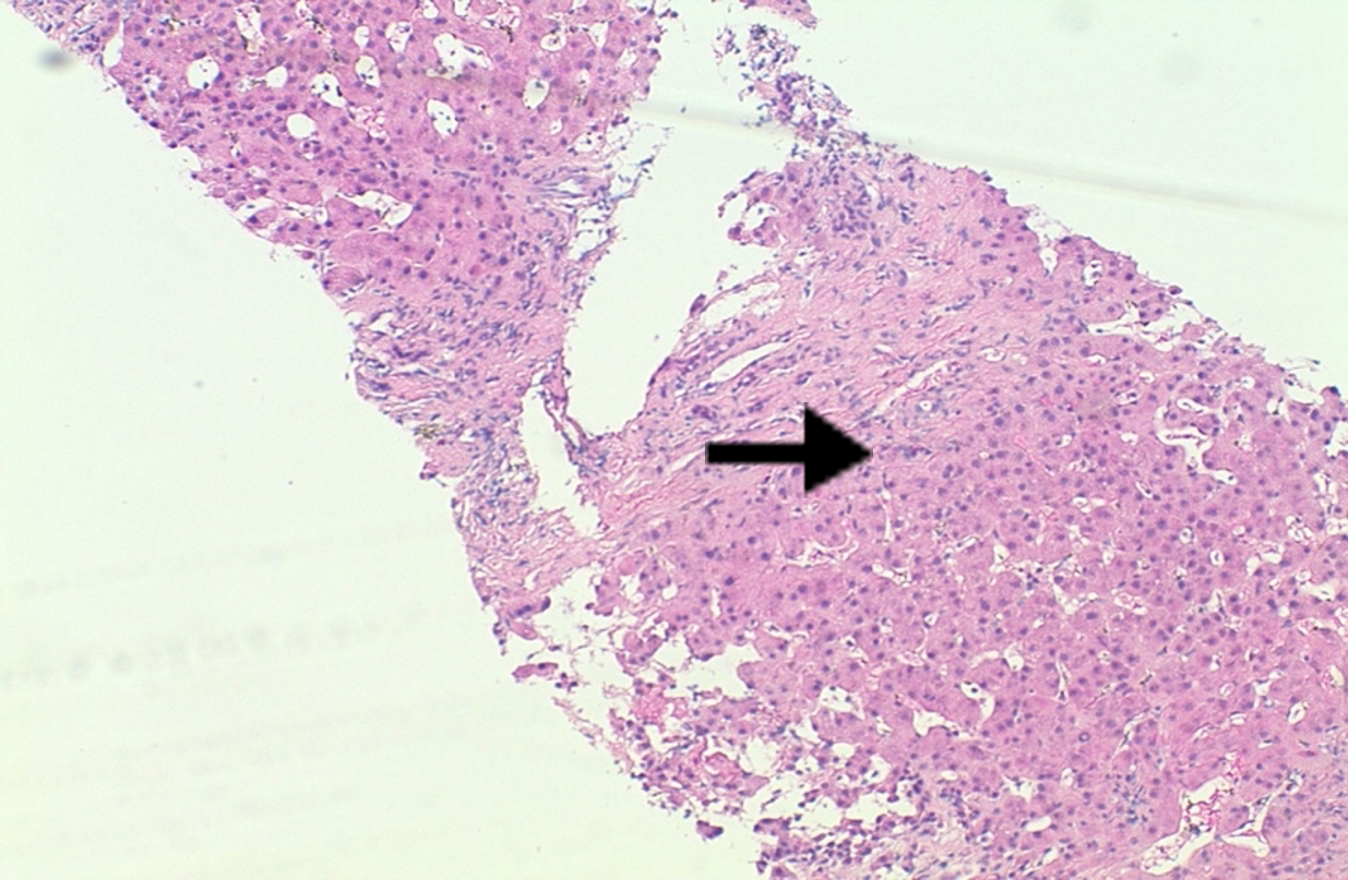
Image 3. Liver biopsy: Iron stain show mesenchymal iron deposition consistent with history of dialysis.
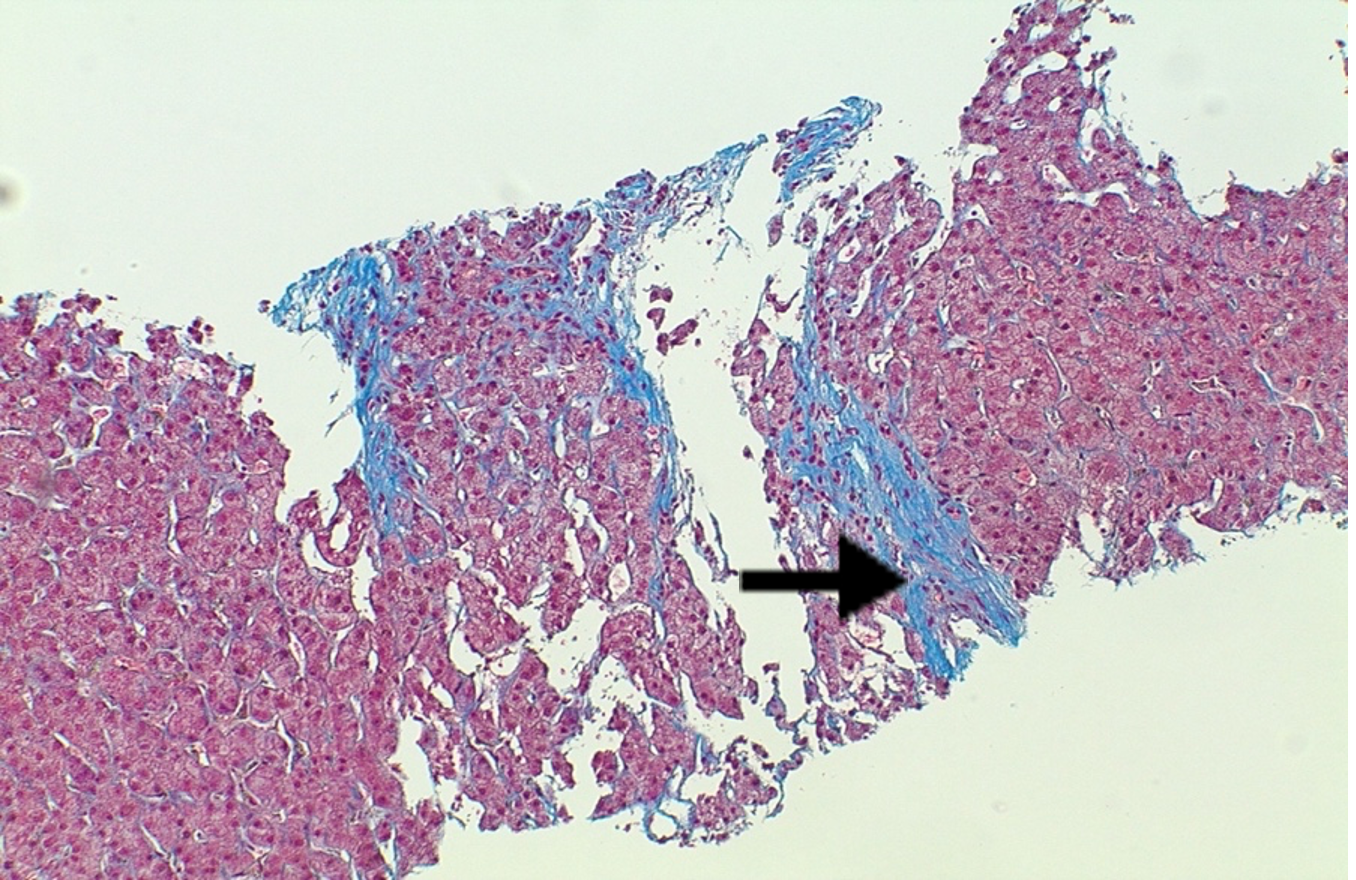
Image 4. Liver biopsy: Trichrome stain highlights sinusoidal dilation, periportal and focal bridging, and focal pericellular fibrosis.
Diagnoses: Cardiac cirrhosis and ascites due to right heart failure from an underlying ASD was diagnosed. Cirrhosis and ascites from cardiac causes is uncommon1, but the key clue to the cause of this patient’s ascites was the elevated peritoneal fluid protein. About 95% of patients with peritoneal fluid protein > 2.5 g/dL are related to cardiac conditions. This finding led to the workup and eventual diagnosis of the patient’s underlying ASD. An ASD is the second most common cardiac congenital abnormality and can be reliably detected with a bubble study3. A liver biopsy, the gold standard diagnostic test, confirmed cardiac cirrhosis with fibrosis of hepatic veins and sinusoids.
Treatment and management. Unfortunately, cardiac medications for cardiac cirrhosis could not be initiated due to hypotension. Instead, he was started on midodrine at the time of discharge. After multiple thoracentesis, a long-term pleural fluid catheter drain was placed with resolution of his pleural effusions on discharge.
Discussion. Cirrhosis of the liver typically results from chronic viral hepatitis, alcohol abuse, medications, or cryptogenic reasons. One etiology that is uncommon is cardiac cirrhosis1, which results from congestive hepatopathy secondary to right heart failure. The prevalence of cardiac cirrhosis has been hard to determine as patients can be asymptomatic and/or have other comorbidities that can result in liver dysfunction1. This patient case highlights the challenges of diagnosing cardiac cirrhosis in a patient with right heart dysfunction complicated by an atrial septal defect with a left to right shunt. Commonly, cardiac cirrhosis is caused by valvular diseases such as TR causing right ventricular systolic dysfunction (RVSD)4.
Although moderate TR and RVSD are evident in this case, it is also complicated by the left to right intra-atrial shunt which increases right sided pressures. This shunt likely added an additional pre-load burden to the central venous system, causing worsening hepatic congestion and resulting in cardiac cirrhosis. This case illustrates the importance of the ascites protein in the evaluation of cirrhosis with ascites and the workup of an elevated ascites protein as a clue to cardiac cirrhosis.
- Rodriguez Ziccardi M, Pendela VS, Singhal M. Cardiac cirrhosis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; July 18, 2022.
- Hernaez R, Hamilton JP. Unexplained ascites. Clin Liver Dis (Hoboken). 2016;7(3):53-56. doi:10.1002/cld.537.
- Pillarisetti J, Nath J, Berenbom L, Lakkireddy D. Cardiac cirrhosis: a rare manifestation of an uncorrected primum atrial septal defect. J Cardiovasc Med (Hagerstown). 2010;11(9):689-691. doi:10.2459/JCM.0b013e3283324730
- Asrani SK, Asrani NS, Freese DK, et al. Congenital heart disease and the liver. Hepatology. 2012;56(3):1160-1169. doi:10.1002/hep.25692
- Blumgart HL, Katzin H. "Cardiac cirrhosis" of the liver: a clinical and pathological study. Trans Am Clin Climatol Assoc. 1938;54:82-86.
- El Hadi H, Di Vincenzo A, Vettor R, Rossato M. Relationship between heart disease and liver disease: a two-way street. Cells. 2020;9(3):567. doi:10.3390/cells9030567
- Estruch R, Fernández-Solá J, Sacanella E, Paré C, Rubin E, Urbano-Márquez A. Relationship between cardiomyopathy and liver disease in chronic alcoholism. Hepatology. 1995;22(2):532-538.
- Pudil, R, Pelouch R, Praus R, Vasatova M, Hulek P, Heart failure in patients with liver cirrhosis. Cor et Vasa. 2013;55(4): 391-396.
- Pozzi M, Carugo S, Boari G, et al. Evidence of functional and structural cardiac abnormalities in cirrhotic patients with and without ascites. Hepatology. 1997;26(5):1131-1137. doi:10.1002/hep.510260507.
- Bochnakova T. Hepatic venous pressure gradient. Clin Liver Dis (Hoboken). 2021;17(3):144-148. doi:10.1002/cld.103