
Pearls of Wisdom: Treating Refractory Acne
Allison is a 26-year-old woman who has an appointment for a flu shot. You immediately notice her prominent facial acne—with scars, pitting, and a moderate degree of inflammation.
She said that she has had acne since telarche, and that she has tried “everything under the sun” with only modest improvement.
Because of a prior deep vein thrombosis, she cannot take oral contraceptives, but she has tried several antibiotics, benzoyl peroxide, retinoic acid, adapalene, tazarotene, and various combinations of these medicines. She has largely given up on the acne ever getting much better and now only follows a maintenance regimen.
Because she has acne on her back and chest, another physician had evaluated her for hyperandrogenism, but that evaluation had failed to show any elevation of adrenal or ovarian androgens. Although there are a few additional treatments available, she is currently uninsured and cannot afford to see a dermatologist.
For a young woman with moderately severe inflammatory acne, is there anything else that a primary care clinician might offer?
A. Spironolactone
B. Combination antibiotics
C. Progestin-only contraceptives
D. High-soy diet
What is the correct answer?
(Answer and discussion on next page)
Louis Kuritzky, MD, has been involved in medical education since the 1970s. Drawing upon years of clinical experience, he has crafted each year for almost 3 decades a collection of items that are often underappreciated by clinicians, yet important for patients. These “Pearls of Wisdom” often highlight studies that may not have gotten traction within the clinical community and/or may have been overlooked since their time of publishing, but warrant a second look.
Now, for the first time, Dr Kuritzky is sharing with the Consultant360 audience. Sign up today to receive new advice each week.
Answer: Spironolactone
The patient has signs of androgenic acne, sometimes also labeled postadolescent acne, based upon the observation that that typical adolescent acne that accompanies the evolution of puberty usually disappears by late adolescence. The primary acne-inducing culprit appears to be androgens, which induce proliferation of the keratin cells lining the sebaceous glands, thereby plugging the orifice of the sebaceous gland and inducing a whitehead or blackhead. Skin flora, once trapped within a plugged sebaceous gland, cause inflammation, cysts, and pustules.
Making the Diagnosis
The symptom complex of persistent, postadolescent acne in a young woman, with acne eruptions not only on her face but also on her back and chest, suggests excessive androgen effect. A previous clinician was wise to look for hyperandrogenism by measuring dehydroepiandosterone sulfate (a measure of adrenal androgens) and total testosterone (a measure of ovarian androgens). Because both values were normal, we can be confident that the patient has neither congenital adrenal hyperplasia nor a testosterone-producing ovarian tumor.
The problem is, however, that the presence of postadolescent acne is generally a reflection of either excessive testosterone or excessive sensitivity to normal levels of testosterone (which may also sometimes manifest as hirsutism in eugonadal women).
Treatment Options
All combination oral contraceptives improve acne in women via several mechanisms:
- Estrogen increases sex hormone binding globulin, which ties up testosterone, leaving less free testosterone to incite keratin cell proliferation.
- Estrogen has direct effects at reducing ovarian testosterone.
- Although most progestins possess some degree of androgenicity, newer progestins (eg, drospirenone) have anti-androgenic activity. Indeed, head-to-head trials comparing drospirenone-containing combination contraceptives show superior efficacy for acne than comparator contraceptives with “traditional” progestins.
Combination oral contraceptives would likely be an efficacious choice for this patient, but because of her history of deep vein thrombosis, they are contraindicated. Is there something else that might be helpful?
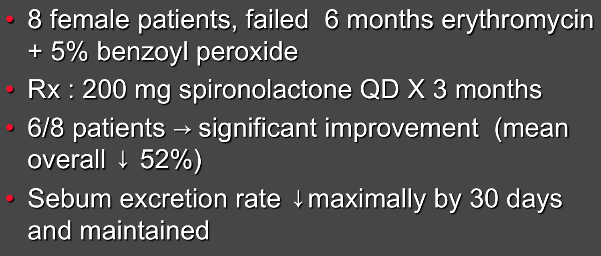
Spironolactone For Resistant Acne1
Spironolactone
Clinicians are used to thinking of spironolactone as an antihypertensive agent, often used for resistant hypertension or as a diuretic in patients with advanced liver disease and ascites. Spironolactone, in addition to being an aldosterone antagonist, blocks androgen receptors at various tissue sites, hence its association (albeit uncommon) with gynecomastia and erectile dysfunction in men.
It has been reported that spironolactone has additional anti-androgenic mechanisms, including reduction in adrenal production of androstenedione and increased clearance of testosterone.
In any case, the anti-androgen effects of spironolactone may be useful in otherwise refractory acne, especially in patients for whom oral contraceptives are contraindicated. Although the studies have generally been small, they consistently show acne improvement in patients who have failed other traditional regimens.
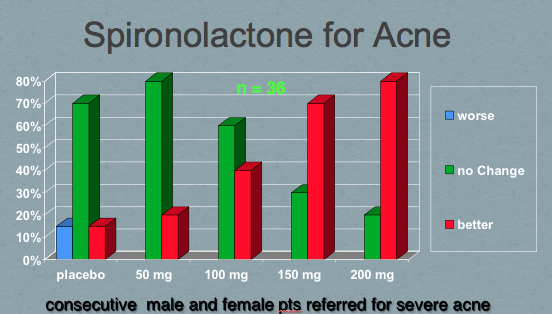
Spironolactone for Acne2
Spironolactone rarely causes hyperkalemia unless coadministered with another potassium-sparing agent (eg, angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers). Nonetheless, it is wise to obtain a baseline potassium level and monitor periodically for hyperkalemia.
What’s the “Take Home”?
After trying a number of interventions, patients sometimes settle for suboptimal disease control. Spironolactone is an inexpensive generic oral agent that is generally well tolerated and modulates one of the fundamental defects leading to acne: testosterone stimulation. Response is usually seen within 1 to 3 months. Although the case described was that of a woman, testosterone is a culprit in men and women alike and has been used successfully in both genders to treat refractory acne.
References:
- Burke BM, Cunliffe WJ. Oral spironolactone therapy for female patients with acne, hirsutism or androgenic alopecia. Br J Dermatol. 1985;112(1):124-125.
- Goodfellow A, Alaghband-Zadeh J, Carter G, et al. Oral spironolactone improves acne vulgaris and reduces sebum excretion. Br J Dermatol. 1984;111(2):209-214.