
Pearls of Wisdom: Migraine With Aura
Jennifer is a 26-year-old woman seeking care for migraine. She describes suffering from 4 to 6 headaches per month, which fulfills the criteria for classic migraine (migraine with aura). Her headaches usually last 4 to 6 hours, but she also experiences problematic prodrome and postdrome with the headaches, in addition to aura.
She specifically requests butalbital/acetaminophone/caffeine (Fioricet) and oxycodone/acetaminophen (Percocet), saying that these are the only 2 medications that have been highly effective for her. She cannot afford triptans.
Jennifer has recently been released from a 2-year prison stint for cocaine dealing and is a former heroin addict, as corroborated by multiple scars on both of her arms. Although she has had past legal and social problems, Jennifer has been upfront about her history and strikes you as sincere and trustworthy.
Which of the following agents might be useful to consider as a migraine preventative agent for this patient?
A. Carisoprodol
B. Bultalbital/acetaminophen/caffeine
C. Riboflavin (vitamin B2)
D. Niacin (vitamin B3)
How do you advise your patient?
(Answer and discussion on next page)
Louis Kuritzky, MD, has been involved in medical education since the 1970s. Drawing upon years of clinical experience, he has crafted each year for almost 3 decades a collection of items that are often underappreciated by clinicians, yet important for patients. These “Pearls of Wisdom” often highlight studies that may not have gotten traction within the clinical community and/or may have been overlooked since their time of publishing, but warrant a second look.
Now, for the first time, Dr Kuritzky is sharing with the Consultant360 audience. Sign up today to receive new advice each week.
Answer: Riboflavin (vitamin B2)
Despite the fact that Jennifer has had her fair share of life difficulties, perhaps she is now reformed. She has not tried to hide her history, but the clinician is still wise to be cautious, especially when a patient asks for substances that can be abused by brand name. Some clinicians prefer to request a urine drug screen prior to initiating any controlled substance. Providing this screen routinely—as opposed to for select patients (eg, patients with tattoos, unconventional dress, or style)—obviates any reason for the particular patient to believe he or she is singled out due to her past.
It is troublesome that Jennifer specifically requests 2 agents that are near the top of the list of abused drugs: Fioricet and Percocet. However, delving into her history further, you learn that she had access to these agents as they were smuggled into the prison. While she found to be particularly effective, she has not used them since her release.
______________________________________________________________________________________________________________________________________________
RELATED CONTENT
Migraine Associated With Structural Brain Changes
When Are OTC Analgesics Appropriate for Acute Migraine
______________________________________________________________________________________________________________________________________________
Treatment Options
Opioid analgesia is a reasonable treatment to abort migraine headache, but not for chronic prophylaxis, as is the case with Jennifer due to the frequency and severity of her headaches. If you were to prescribe an opioid for rescue medication (and I am not suggesting that you should), it would probably be wiser to use an opioid with a less notorious street name. (Sidenote: One patient that I know was in Walmart, placed his prescription bag in the upper shelf of the shopping cart, and looked away for a minute—long enough for his prescription for Ritalin to be stolen out of the cart. Security cameras captured the theft. Maybe the thieves would have also stolen tetracycline with equal speed and dexterity, but I doubt it.)
Fioricet is another popular substance on the street. Butalbital, a rapid-acting, highly reinforcing barbiturate, is one of its components, and has never been shown to provide improved headache relief beyond what is provided by the other 2 active ingredients—acetaminophen and caffeine. Given that there is no evidence in support of the efficacy of butalbital for migraine, contrasted with ample evidence of its abuse potential, it is difficult to justify use of Fioricet as a primary tool for management of migraine.
So, until we gain more experience with Jennifer, it might be better to stick with agents that have little or no abuse potential. Riboflavin (vitamin B2) is such a substance.
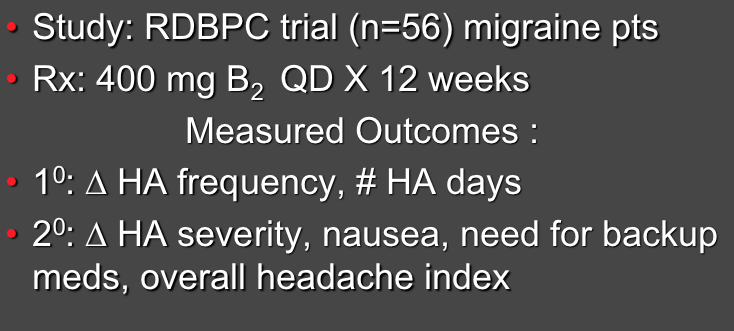
Study: Migraine Prophylaxis with Riboflavin1
Literature
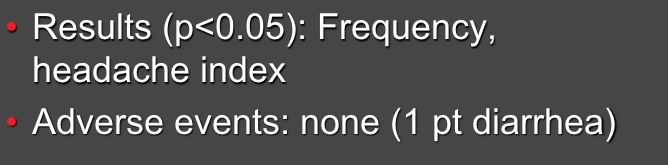
In a randomized double-blind placebo controlled trial, Schoenen et al1 found that riboflavin had a statistically significant impact upon migraine headache. Riboflavin was chosen based upon the premise that it might enhance mitochondrial energy efficiency, which has been noted to be suboptimal in migraineurs between attacks. Additionally, a pilot trial of riboflavin for migraine had found favorable results.
The dose of riboflavin was fairly high (400 mg/d), and although there is no serious known toxicity related to riboflavin, 1 patient did experience diarrhea that may have been related to the riboflavin. Additionally, positive effects of riboflavin were seen most prominently in the final month of the 3-month trial. Hence, clinicians should inform patients that full potential benefits of riboflavin may take some time to manifest.
Results: Migraine Prophylaxis with Riboflavin1
What’s the “Take Home”?
Migraine headaches can be disabling. Just because a patient has had substance misuse problems in the past does not preclude administration of controlled substances appropriate for treatment. However, if other potentially effective agents are available that lack abuse potential, they may be preferred. In this case, riboflavin may be a reasonable prophylaxis agent to fit the bill.
Reference:
1. Schoenen J, Jacquy J, Lenaerts M. Effectiveness of high-dose riboflavin in migraine prophylaxis. A randomized controlled trial. Neurology. 1998;50(2):4.