
Young Woman With Abdominal Pain and Fullness
 A 23-year-old woman presents with weight loss, epigastric pain, abdominal fullness, and mild nausea. She reports that she has had a slow-growing mass on her upper middle abdomen. She denies vomiting and does not have evidence of jaundice. The only significant finding in her medical history is a myringotomy performed many years earlier. She currently takes an oral contraceptive.
A 23-year-old woman presents with weight loss, epigastric pain, abdominal fullness, and mild nausea. She reports that she has had a slow-growing mass on her upper middle abdomen. She denies vomiting and does not have evidence of jaundice. The only significant finding in her medical history is a myringotomy performed many years earlier. She currently takes an oral contraceptive.
A firm, nontender, epigastric, midline mass is noted in this wellnourished patient. Laboratory values, including a complete blood cell count and the results of liver function tests and pancreatic enzyme measurement, are normal.
 A CT scan with contrast of the abdomen reveals a well-defined mass arising from the inferior aspect of the head of the pancreas at the Oddi sphincter (Figure 1). The tumor has both solid and cystic components, with diffuse, inhomogeneous enhancement and no evidence of calcification. The mass is associated with mild pancreatic and biliary ductal distention. No other abnormalities are noted within the abdomen or lung bases.
A CT scan with contrast of the abdomen reveals a well-defined mass arising from the inferior aspect of the head of the pancreas at the Oddi sphincter (Figure 1). The tumor has both solid and cystic components, with diffuse, inhomogeneous enhancement and no evidence of calcification. The mass is associated with mild pancreatic and biliary ductal distention. No other abnormalities are noted within the abdomen or lung bases.
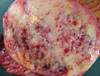
Cystadenoma/carcinoma and a solid-cystic papillary tumor of the pancreas are considered in the differential diagnosis. The patient undergoes an elective partial pancreatoduodenectomy. A well-circumscribed, thickly encapsulated, fleshy, yellow and gray mass (7.5 * 5.3 * 5.0 cm) is removed (Figure 2). Numerous cysts (the largest is 0.2 cm) are scattered throughout the specimen; the remaining cut surfaces have a fine granular appearance. Although the pancreatic duct is occluded 0.3 cm into the specimen, the surgical margins (distal pancreatic margins, bile duct margin, and distal and proximal small intestinal margins) are free of tumor.
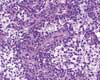 Histologic examination reveals that most of the encapsulated pancreatic neoplasm excised from this patient has sheets of intermediate-sized cells with ovoid to irregular nuclei; fine heterochromatin; small nucleoli; and moderate amounts of pink to clear, occasionally vacuolated cytoplasm (Figure 3). Numerous small foci of necrobiotic cells with pyknotic nuclei and hypereosinophilic cytoplasm are also present.
Histologic examination reveals that most of the encapsulated pancreatic neoplasm excised from this patient has sheets of intermediate-sized cells with ovoid to irregular nuclei; fine heterochromatin; small nucleoli; and moderate amounts of pink to clear, occasionally vacuolated cytoplasm (Figure 3). Numerous small foci of necrobiotic cells with pyknotic nuclei and hypereosinophilic cytoplasm are also present.
The tumor is invested by a rich capillary network, with cells radially arranged around minute fibrovascular stocks, which resemble rosettes and pseudopapillae. Extensive hemorrhage and degeneration resulted in pseudomicrocysts devoid of an epithelial lining. Fewer than one mitosis (with both perineural and lymphangitic invasion) per high-power field is noted within the tumor. The remaining pancreas shows evidence of chronic pancreatitis; the small intestine (duodenum) is unremarkable.
The patient's recovery is uneventful. At follow-up 2 years after the procedure, a CT scan demonstrates no evidence of recurrent tumor. She is not required to take insulin; there is no evidence of malabsorption.
SOLID-CYSTIC PAPILLARY TUMOR: AN OVERVIEW
Epidemiology. Solid-cystic papillary tumor of the pancreas—also known as papillary solid and/or cystic neoplasm, papillary epithelial tumor, and solid-pseudopapillary tumor—is a rare neoplasm of uncertain malignant potential that is found almost exclusively in young women, especially adolescents. Since its original description by Frantz in 1959, more than 400 cases have been documented in the literature.1 Tumors of up to 20 cm in diameter have been reported.2
Pathogenesis. The histogenesis of the solid-cystic papillary tumor remains illusive, despite extensive immunohistochemical staining and electron microscopy studies. A ductal cell origin has been hypothesized, because of the absence of zymogen and neurosecretory granules on electron microscopy.3
Positive immunohistochemical staining for α1-antitrypsin and α1- antichymotrypsin suggests an acinar cell origin.4,5 However, α1-antitrypsin immunoreactivity is nonspecific to pancreatic exocrine cells.
Another theory suggests that the tumor has an endocrine origin; this is based on the observation of neurosecretory granules by electron microscopy and immunohistochemical staining of certain pancreatic hormones, including glucagon and insulin, and neuron-specific enolase.6,7 The lack of neurosecretory granules in some cells and the presence in others causes further confusion about the cell of origin. Because of conflicting data and the mixed exocrine and endocrine milieu within the tumor, numerous investigators have proposed that the tumor originates from a multipotential stem cell, which is able to differentiate into and exhibit properties of ductal, acinar, and/or endocrine cells.8
Malignant potential. The tumor can arise anywhere within the pancreas or even in areas of pancreatic heterotopia.9 The neoplasm rarely invades structures but rather displaces them with “pushing borders.” Surgical resection of the tumor, even if large, is often possible.
Most solid-cystic papillary tumors are benign or of low-grade malignancy; however, in one study, 43 of 289 tumors had malignant features, including surrounding tissue infiltration, tumor recurrence, lymph node metastasis, and distant metastasis.2 The prognosis for patients with malignant tumors is not dismal; many persons live more than 5 years after surgery. Benign and malignant tumors share similar histologic and immunohistochemical findings; thus, prediction of malignancy and metastatic potential is difficult.
Pathologic findings. Solid areas of the tumor contain sheets and cords of cells arranged around delicate fibrovascular septa. Microcystic spaces and discohesion between cells farthest from the rich capillary network result in a pseudopapillary pattern and pseudorosette formation. Myxoid degeneration, cystic areas, aggregates of foamy histiocytes, hemorrhage, and hyalinization of blood vessels are often striking. Cystic degeneration is thought to evolve from vascular compromise within the tumor; however, small tumors (2 cm in diameter) have shown cystic properties.
Tumor cells are small to medium- sized and cuboid or polygonal. The chromatin pattern is often fine with inconspicuous nucleoli and indented or folded nuclei. Cell cytoplasm often varies from eosinophilic to clear to basophilic. Periodic acid- Schiff–positive hyaline globules may be numerous. Mitoses are usually rare, and the circumscribed tumor is often encapsulated by thick fibrous connective tissue. Vascular invasion is a rare but worrisome finding suggestive of malignant behavior.