
Lambl Excrescences in a Woman With Recurrent Strokes
A 47-year-old woman presented with altered mental status and slurred speech. Past medical history included hypertension, multiple strokes, and alcohol- induced pancreatitis. The patient frequently used cocaine. Initial blood pressure was 198/116 mm Hg. A urine drug screen was positive for cocaine. The neurological findings evolved over 12 hours to include further slurring of speech, leftward tongue deviation, left facial droop, and left-sided hemiparesis.
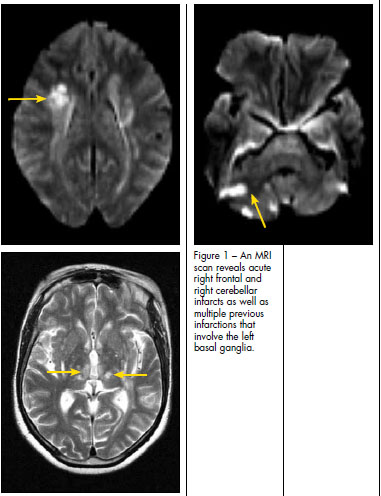 A CT scan of the head revealed several age-indeterminate lacunar infarcts and generalized atrophy. An MRI scan (Figure 1) showed acute right frontal and right cerebellar infarcts as well as multiple previous infarctions. Because of the patient's history of recurrent cerebrovascular events, additional studies were ordered. The results of carotid artery ultrasonography and transthoracic echocardiography were normal. However, transesophageal echocardiography demonstrated Lambl excrescences along coaptation points on the aortic valve (Figure 2).
A CT scan of the head revealed several age-indeterminate lacunar infarcts and generalized atrophy. An MRI scan (Figure 1) showed acute right frontal and right cerebellar infarcts as well as multiple previous infarctions. Because of the patient's history of recurrent cerebrovascular events, additional studies were ordered. The results of carotid artery ultrasonography and transthoracic echocardiography were normal. However, transesophageal echocardiography demonstrated Lambl excrescences along coaptation points on the aortic valve (Figure 2).
LAMBL EXCRESCENCES: AN OVERVIEW
Lambl excrescences (sometimes also called valvular strands or papillary fibroelastomas) are small, filiform processes located at lines of closure on cardiac valves (usually at the aortic and mitral valves). The lesions—a product of repeated trauma consequent to forceful closure1,2— are thought to result from organized thrombi that form at the contact margins of the valves. Theexcrescences are likely a contingent of valve "aging" or "wear and tear" from shear forces, endothelial tears, and localized thrombus formation. In the majority of reported cases, patients with Lambl excrescences are asymptomatic, but they may present with cerebral ischemia, presumably from emboli.3,4 Treatment has been either medical (anticoagulation) or surgical (usually valve "cleaning" or shaving off of the lesions) if emboli are presumed secondary to them.1 This patient presented with Lambl excrescences and recurrent cerebral ischemic events. The clinical dilemma was whether the ischemic pathology was a result of the excrescences or other critical risk factors.
OUTCOME OF THIS CASE
This patient had other risk factors for recurrent strokes—cocaine use and hypertension. She agreed to stop using cocaine. Warfarin was prescribed, but the patient was not adherent with therapy. A shaving off of her Lambl excrescences was accomplished with surgery. Unfortunately, she used cocaine again, became severely hypertensive, and experienced another stroke. This pattern suggested her recurrent ischemic events were either multifactorial or unrelated to Lambl excrescences.

1. Aziz F, Baciewicz FA Jr. Lambl’s excrescences: review and recommendations. Tex Heart Inst J.
2007;34:366-368.
2. Aggarwal A, Leavitt BJ. Images in clinical medicine. Giant Lambl’s excrescences. N Engl J Med. 2003;349:e24.
3. Wolf RC, Spiess J, Vasic N, Huber R. Valvularstrands and ischemic stroke. Eur Neurol. 2007;57:
227-231.
4. Walpot J, Hans Pasteuning W, Koeman J, Volker P. Papillary fibroelastoma of the aortic valve:
a rare cause of stroke. Eur J Echocardiogr. 2007;8: 489-491.