
A Case of Concerning Crepitus
 A 72-year-old man presents to the emergency department (ED) after a violent assault. He complains of facial, neck, and chest pain with odynophagia and hoarseness. He did not lose consciousness, and he denies dyspnea, epistaxis, cough, and hemoptysis. His past medical history includes gastroesophageal reflux disease and previous right shoulder and right knee surgery.
A 72-year-old man presents to the emergency department (ED) after a violent assault. He complains of facial, neck, and chest pain with odynophagia and hoarseness. He did not lose consciousness, and he denies dyspnea, epistaxis, cough, and hemoptysis. His past medical history includes gastroesophageal reflux disease and previous right shoulder and right knee surgery.
PHYSICAL EXAMINATION
Heart rate is 90 beats per minute; blood pressure, 149/76 mm Hg; and oxygen saturation on room air, 97%. A small laceration is noted in the superior portion of the right eyebrow with right periorbital ecchymosis. No hemotympanum or nasal septal hematomas are visible, and there are no signs of oral or dental trauma. Crepitus is palpable in the soft tissue of his head, neck, and thorax, and tenderness to palpation is noted over the right anterior chest wall. His trachea is midline, and equal breath sounds are audible bilaterally on auscultation. Neurological examination is unremarkable.
LABORATORY AND IMAGING RESULTS
White blood cell (WBC) count is 13,000/μL; hematocrit, 40%; and platelet count, 278,000/μL. Results of a chemistry panel are unremarkable. Urinalysis shows no evidence of hematuria or infection, but a urine toxicology screen is positive for amphetamines. CT scans of the head, face, and cervical spine reveal nasal bone fractures as well as subcutaneous air in the soft tissues of the right cheek, neck, and chest. A CT scan of the abdomen shows no evidence of acute intra-abdominal injury. A chest radiograph (A) obtained on admission to the ED is normal. A subsequent CT scan of the chest (B), obtained 2 hours later, reveals air in the anterior mediastinum and cervical region. No bronchopleural tear is visualized radiologically despite 3-dimensional (3-D) reconstruction.
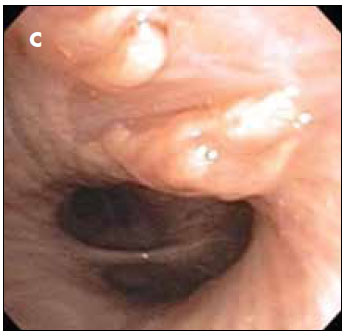
An esophagogram shows no extravasation of contrast material that would suggest esophageal injury. Ear, nose, and throat evaluation does, however, reveal laryngeal soft tissue injury with likely resultant right vocal paralysis. Flexible bronchoscopy is performed (C). CASE DISCUSSION
CASE DISCUSSION
The initial radiograph showed no evidence of rib fractures, pneumothorax, or pneumomediastinum. However, the chest CT scan obtained 2 hours later demonstrated a pneumomediastinum that prompted urgent bronchoscopy. Flexible bronchoscopy revealed a slit-like tear 2 cm distal to the carina on the medial wall of the right main bronchus (see Figure). It was not possible to ascertain whether the tear represented an intimal flap or was of full thickness. No cardiothoracic surgical repair was attempted in light of the patient’s continued clinical and radiological improvement while under close in-hospital observation. The patient remained afebrile with a normal WBC count.
TRACHEOBRONCHIAL WALL INJURIES: AN OVERVIEW
Clinical features. Despite their rarity, tracheobronchial wall injuries necessitate early recognition in order to minimize morbidity and mortality.1-4 The reported incidence in patients who have sustained blunt trauma is between 0.13% and 5.4%.1,5 Such injuries are usually located within 2.5 cm of the carina and occur more frequently in the right mainstem bronchus.6 These ruptures can be transverse, longitudinal, or complex.7 Patients can present with variable symptoms ranging from vague chest pains and breathlessness to hemoptysis and stridor.8 Causes. Although high-speed motor vehicle accidents are the most common cause of a tracheobronchial tear, such injuries can also result from hanging, falls, and even endotracheal intubation.5,9 In car accidents, the acceleration-deceleration injury to the bronchi is secondary to the movement of the large airways around a fixed position at the carina. In crush injuries, the resultant increased transverse diameter of the chest causes a tearing of the distal trachea and main bronchi as they are pulled laterally.10-13 This patient sustained a disruption to his right mainstem bronchus from blunt force trauma with pneumomediastinum in the absence of a pneumothorax. Diagnostic studies. Kunisch-Hoppe and colleagues14 found that contrast media–enhanced thoracic CT demonstrated disappointing results in the diagnosis of tracheobronchial disruptions compared with flexible bronchoscopy.
 Thus, flexible bronchoscopy is considered the gold standard for identifying such an injury.1,6,14 The advent of chest CT with 3-D reconstruction of the tracheobronchial tree may also enable similar diagnoses; however, its sensitivity is unknown.15 This case of tracheobronchial disruption was diagnosed on the basis of flexible bronchoscopy alone. Radiological clues such as persistent pneumothoraces despite chest tube placement, “fallen lung” sign (which describes lung collapse laterally away from the hilum attributable to disruption of the normal hilar attachments of the affected lung), progressive pneumomediastinum and/or subcutaneous emphysema, focalperibronchial air collections, focal bronchial wall irregularities, or abnormal position of an endotracheal tube or an overdistended balloon may suggest a tracheobronchial disruption and the need for prompt flexible bronchoscopy. However, up to 10% of patients have no radiological evidence of tracheobronchial wall injuries.6,12,16 In a patient with a suspected tracheobronchial tear, flexible bronchoscopy should be performed only by an experienced bronchoscopist6,8 to reduce the risk of iatrogenic injury. In addition, missing a tracheobronchial tear can increase both mortality1-4 and morbidity (by 10% to 25%)17 because of the resulting complications of recurrent pneumonia, mediastinitis, and possibly atelectasis.8,18,19 Under these circumstances, Le Guen and associates8 suggest that multi-detector CT with high spatial resolution images of the whole lung without any anatomical gap, together with 3-D reconstruction, may change diagnostic strategies in patients with blunt chest trauma, especially in decisions involving the need for flexible bronchoscopy. Treatment. Although primary repair of a tracheobronchial wall injury can yield good results,11,19 nonoperative management can also be successful without subsequent complications, especially in stable patients who have tracheobronchial tears of 0.9 to 3 cm in length.1,10,20 Surgery, however, is recommended for patients with progressive respiratory subcutaneous emphysema, increasing oxygen requirements, and persistent non-approximation of the wound edges.21,22
Thus, flexible bronchoscopy is considered the gold standard for identifying such an injury.1,6,14 The advent of chest CT with 3-D reconstruction of the tracheobronchial tree may also enable similar diagnoses; however, its sensitivity is unknown.15 This case of tracheobronchial disruption was diagnosed on the basis of flexible bronchoscopy alone. Radiological clues such as persistent pneumothoraces despite chest tube placement, “fallen lung” sign (which describes lung collapse laterally away from the hilum attributable to disruption of the normal hilar attachments of the affected lung), progressive pneumomediastinum and/or subcutaneous emphysema, focalperibronchial air collections, focal bronchial wall irregularities, or abnormal position of an endotracheal tube or an overdistended balloon may suggest a tracheobronchial disruption and the need for prompt flexible bronchoscopy. However, up to 10% of patients have no radiological evidence of tracheobronchial wall injuries.6,12,16 In a patient with a suspected tracheobronchial tear, flexible bronchoscopy should be performed only by an experienced bronchoscopist6,8 to reduce the risk of iatrogenic injury. In addition, missing a tracheobronchial tear can increase both mortality1-4 and morbidity (by 10% to 25%)17 because of the resulting complications of recurrent pneumonia, mediastinitis, and possibly atelectasis.8,18,19 Under these circumstances, Le Guen and associates8 suggest that multi-detector CT with high spatial resolution images of the whole lung without any anatomical gap, together with 3-D reconstruction, may change diagnostic strategies in patients with blunt chest trauma, especially in decisions involving the need for flexible bronchoscopy. Treatment. Although primary repair of a tracheobronchial wall injury can yield good results,11,19 nonoperative management can also be successful without subsequent complications, especially in stable patients who have tracheobronchial tears of 0.9 to 3 cm in length.1,10,20 Surgery, however, is recommended for patients with progressive respiratory subcutaneous emphysema, increasing oxygen requirements, and persistent non-approximation of the wound edges.21,22
OUTCOME OF THIS CASE
In view of this patient’s clinical stability and the likelihood that the tracheobronchial injury was not a full-thickness tear, conservative treatment was chosen. The patient was eventually discharged home after recovery from his injuries.
1. Kuhne CA, Kaiser GM, Flohe S, et al. Nonoperative management of tracheobronchial injuries in severely injured patients. Surg Today. 2005;35:518-523.
2. Bertelsen S, Howitz P. Injuries of the trachea and bronchi. Thorax. 1972;27: 188-194.
3. Devitt JH, Boulanger BR. Lower airway injuries and anaesthesia. Can J Anaesth. 1996;43:148-159.
4. Shorr RM, Crittenden M, Indeck M, et al. Blunt thoracic trauma. Analysis of 515 patients. Ann Surg. 1987;206:200-205.
5. Huh J, Milliken JC, Chen JC. Management of tracheobronchial injuries
following blunt and penetrating trauma. Am Surg. 1997;63:896-899.
6. Hardin KA, Louie S. Occult tracheobronchial injury: a subsegmental location.
J Bronchol. 2002;9:290-293.
7. Symbas PN, Justicz AG, Ricketts RR. Rupture of the airways from blunt trauma:
treatment of complex injuries. Ann Thorac Surg. 1992;54:177-183.
8. Le Guen M, Beigelman C, Bouhemad B. Chest computed tomography with multiplanar reformatted images for diagnosing traumatic bronchial rupture: a case report. Crit Care. 2007;11:R94.
9. Rossbach MM, Johnson SB, Gomez MA, et al. Management of major tracheobronchial injuries: a 28-year experience. Ann Thorac Surg. 1998;65:182-186.
10. Wisner DH. Trauma to the chest. In: Sabiston DC Jr, Spencer FC, eds. Surgery of the Chest. 6th ed. Philadelphia: WB Saunders; 1995:456-493.
11. Stewart BT, Meridew CG, Krishnan M. Post traumatic rupture of the right main bronchus: a rare clinical entity? J R Coll Surg Edinb. 1999;44:132-133.
12. Tull DF, Hailstone D, Fulda GJ, Giberson F. Tracheobronchial disruption following low-energy trauma. J Emerg Med. 1996;14:579-583.
13. Hemmila MR, Hirschl RB, Teitelbaum DH, et al. Tracheobronchial avulsion and associated innominate artery injury in blunt trauma: case report and literature review. J Trauma. 1999;46:505-512.
14. Kunisch-Hoppe M, Hoppe M, Rauber K, et al. Tracheal rupture caused by blunt chest trauma: radiological and clinical features. Eur Radiol. 2000;10:480-483.
15. Mirvis SE. Imaging of acute thoracic injury: the advent of MDCT screening. Semin Ultrasound CT MR. 2005;26:305-331.
16. Kuhlman JE, Pozniak MA, Collins J, Knisely BL. Radiographic and CT findings of blunt chest trauma: aortic injuries and looking beyond them. Radiographics. 1998;18:1085-1106; discussion 1107-1108; quiz 1.
17. Huang J, Needs RE, Miller HA, Devitt JH. Unsuspected tracheal rupture in blunt thoracic trauma. Can J Anaesth. 1994;41:1208-1210.
18. Barmada H, Gibbons JR. Tracheobronchial injury in blunt and penetrating chest trauma. Chest. 1994;106:74-78.
19. Cassada DC, Munyikwa MP, Moniz MP, et al. Acute injuries of the trachea and major bronchi: importance of early diagnosis. Ann Thorac Surg. 2000;69: 1563-1567.
20. Hager J, Gunkel AR, Riccabona U. Isolated longitudinal rupture of the posterior tracheal wall following blunt neck trauma. Eur J Pediatr Surg. 1999;9:104-108.
21. Neef H. Tracheobronchial injuries in blunt thoracic trauma [in German]. Zentralbl Chir. 1997;122:674-680.
22. Corsten G, Berkowitz RG. Membranous tracheal rupture in children following minor blunt cervical trauma. Ann Otol Rhinol Laryngol. 2002;111 (3, pt 1):197-199.