
Carotid Dissection From Weight Lifting
A 37-year-old man was brought to the emergency department (ED) after he had 2 near-syncopal events. The first occurred in the morning and rapidly resolved; the second occurred later in the day at work. The night before he had a headache and neck pain. In the ED, he reported left arm and leg weakness and was noted to have left facial droop. His medical history was unremarkable. He denied alcohol, cigarette, and illicit drug use. He lifted weights and played racquetball regularly.
 The patient had expressive aphasia. Blood pressure was 133/65 mm Hg; heart rate, 56 beats per minute; respiration rate, 18 breaths per minute; temperature, 37°C (98.6°F); and oxygen saturation, 100% on room air. There were no murmurs, rubs, or gallops and no carotid bruit. The left-sided weakness was accompanied by decreased sensation. Results of laboratory studies and a urinary drug screen were normal.
The patient had expressive aphasia. Blood pressure was 133/65 mm Hg; heart rate, 56 beats per minute; respiration rate, 18 breaths per minute; temperature, 37°C (98.6°F); and oxygen saturation, 100% on room air. There were no murmurs, rubs, or gallops and no carotid bruit. The left-sided weakness was accompanied by decreased sensation. Results of laboratory studies and a urinary drug screen were normal.
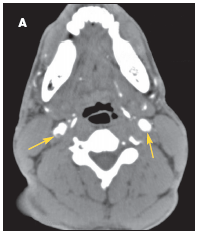
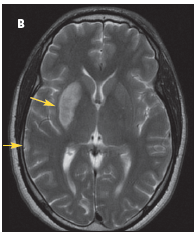
The patient was admitted with a diagnosis of stroke. A CT scan of the brain revealed no bleeding or infarction. A CT angiogram showed bilateral internal carotid dissection, on the right more than the left (A). A heparin drip and aspirin were started. MRI done 24 hours later showed acute infarction in the right basal ganglia and to a smaller degree in the right temporal lobe (B); petechial hemorrhages were noted in the acute infarction. At this point, the heparin drip and aspirin were discontinued. The patient could not be anticoagulated because of the hemorrhagic conversion.
 Results of studies to determine the cause of the stroke, including a transthoracic echocardiogram with bubble study, a hypercoagulability panel, measurement of rheumatoid factor and antinuclear antibody, lupus evaluation panel, and fasting lipid panel, were all normal. Serial CT scans showed mass effect and edema. Intravenous dexamethasone was started.
Results of studies to determine the cause of the stroke, including a transthoracic echocardiogram with bubble study, a hypercoagulability panel, measurement of rheumatoid factor and antinuclear antibody, lupus evaluation panel, and fasting lipid panel, were all normal. Serial CT scans showed mass effect and edema. Intravenous dexamethasone was started.
At discharge, the mass effect and edema had decreased. Intravenous dexamethasone was switched to an oral tapering dose of the corticosteroid, and the patient was transferred to a rehabilitation center.
Carotid dissection associated with sports and other physical activities is an increasingly recognized, although still underestimated, cause of stroke in young patients.1 More research into the pathophysiology and management of this condition is needed given its devastating effect on young lives. Anticoagulation with heparin and warfarin is the accepted standard of treatment. However, a study from the United Kingdom is currently comparing anticoagulation with antiplatelet therapy.2
Sports-related carotid dissection typically occurs in older patients (aged 40 to 45 years).3 Weight lifting—the probable cause in this case—is an uncommon cause of sports-related carotid dissection. The patient was advised to stop this activity. The presyncopal events were probably secondary to bilateral dissection, which is less common than unilateral dissection.3
1. Norris JW, Brandt T. Management of cervical arterial dissection. Int J Stroke. 2006;1:59-64.
2. Cervical Artery Dissection in Stroke Study Trial Investigators. Antiplatelet therapy vs anticoagulation in cervical artery dissection: rationale and design of the Cervical Artery Dissection in Stroke Study (CADISS). Int J Stroke. 2007;2:292-296.
3. Dharmasaroja P, Dharmasaroja P. Sports-related internal carotid artery dissection: pathogenesis and therapeutic point of view. Neurologist. 2008;14:307-311.