
Calciphylaxis
 A55-year-old woman was hospitalized with pain and ulcers on the right breast, fourth digit of the right hand, and left fifth toe. She had hypertension, end-stage renal disease (ESRD) for which she was receiving hemodialysis, atrial fibrillation, and coronary artery disease, and she was morbidly obese (body mass index, 45 kg/m2). Medications included aspirin, metoprolol, atorvastatin, sevelamer, and isosorbide mononitrate. The patient denied using tobacco, alcohol, or illicit drugs. For the past year, she had been taking warfarin only intermittently and had discontinued it altogether a month before presentation.
A55-year-old woman was hospitalized with pain and ulcers on the right breast, fourth digit of the right hand, and left fifth toe. She had hypertension, end-stage renal disease (ESRD) for which she was receiving hemodialysis, atrial fibrillation, and coronary artery disease, and she was morbidly obese (body mass index, 45 kg/m2). Medications included aspirin, metoprolol, atorvastatin, sevelamer, and isosorbide mononitrate. The patient denied using tobacco, alcohol, or illicit drugs. For the past year, she had been taking warfarin only intermittently and had discontinued it altogether a month before presentation.
About 10 days earlier, painful hyperpigmented, violaceous, and indurated plaque-like ulcers with central eschar developed on the patient’s right breast. She had fever and chills while undergoing dialysis, which prompted the hospital admission.
On examination, the patient was afebrile; vital signs were normal. Erythematous 4 cm by 3 cm lesions with induration and a surrounding area of 10 cm by 8 cm erythema were noted on the right breast (A). Similar but smaller lesions were noted on the right fourth digit of the hand and left fifth toe. Abnormal laboratory values were as follows: calcium, 10.1 mg/dL (normal range, 8.5 mg to 10.5 mg/dL); phosphorus, 7.9 mg/dL (normal, 2.6 mg to 4.5 mg/dL); albumin, 3.1 g/dL (normal, 3.3 g to 5 g/dL); and intact parathyroid hormone, 2280 pg/mL (normal, 10 pg to 55 pg/mL).
 Electrocardiographic findings showed atrial fibrillation with a rapid ventricular rate of 160 beats per minute with no ischemic changes. Heart rate was controlled with beta blockers, and myocardial ischemia was ruled out with negative cardiac enzymes. Chest radiograph showed atherosclerotic calcifications of the aortic knob and cardiomegaly. Radiographs of the patient’s hand showed extensive atherosclerotic vascular calcifications (B). Arterial Doppler ultrasonography of the extremities showed right femoral, left ileo-femoral, and right radial and ulnar artery occlusive disease with mild distal ischemia at rest.
Electrocardiographic findings showed atrial fibrillation with a rapid ventricular rate of 160 beats per minute with no ischemic changes. Heart rate was controlled with beta blockers, and myocardial ischemia was ruled out with negative cardiac enzymes. Chest radiograph showed atherosclerotic calcifications of the aortic knob and cardiomegaly. Radiographs of the patient’s hand showed extensive atherosclerotic vascular calcifications (B). Arterial Doppler ultrasonography of the extremities showed right femoral, left ileo-femoral, and right radial and ulnar artery occlusive disease with mild distal ischemia at rest.
Because the patient had no predisposing cardiac conditions and blood cultures were negative, bacterial endocarditis was ruled out. Autoimmune serology was negative. Clinical presentation, high calcium-phosphate product, secondary hyperparathyroidism, and radiographic evidence of vascular calcification were highly suggestive of calciphylaxis. Intravenous fluids and calcitonin were added to the drug regimen, and the sevelamer dosage was increased from 800 mg to 1600 mg, 3 times a day.
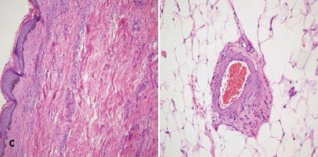 Punch biopsy results of right breast lesions were inconclusive. A subsequent deep tissue biopsy results displayed superficial dermal angiomatosis with chronic inflammation and abundant adipose tissue (C). Technitium-sestamibi scan suggested a left inferior parathyroid adenoma. The patient underwent successful emergent subtotal parathyroidectomy for severe secondary
Punch biopsy results of right breast lesions were inconclusive. A subsequent deep tissue biopsy results displayed superficial dermal angiomatosis with chronic inflammation and abundant adipose tissue (C). Technitium-sestamibi scan suggested a left inferior parathyroid adenoma. The patient underwent successful emergent subtotal parathyroidectomy for severe secondary 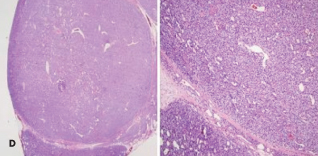 hyperparathyroidism. An examination of a biopsy specimen stained with hematoxylin and eosin (H and E) demonstrated hyperplasia with dystrophic calcification (D). After surgery, the calcium-phosphate product was 20 and parathyroid hormone level 3.8 pg/mL. Pain and skin lesions slowly seemed to be resolving.
hyperparathyroidism. An examination of a biopsy specimen stained with hematoxylin and eosin (H and E) demonstrated hyperplasia with dystrophic calcification (D). After surgery, the calcium-phosphate product was 20 and parathyroid hormone level 3.8 pg/mL. Pain and skin lesions slowly seemed to be resolving.
Calciphylaxis is a rare phenomenon with an estimated incidence of 1% to 4.5% among dialysis patients.1 It was first described as a hypersensitivity reaction after exposure to certain “sensitizers” by Seyle in 1962.2 Small artery medial calcification with endovascular fibrosis leading to low perfusion pressures and the activation of inflammatory mediators with hemodialysis cause endothelial damage resulting in ischemic skin lesions. Distal extremities are involved in 90% of cases. Involvement of breast tissue, trunk, and proximal extremities carries a poorer prognosis.3 Calciphylactic lesions are non-healing and prone to secondary bacterial infections. Mortality approaches 80% without treatment. Systemic calciphylaxis can result in painful ischemic myopathy with muscle weakness
and/or severe myositis.4
Risk factors for calciphylaxis include obesity, female gender, Caucasian race, low albumin levels, elevated serum alkaline phosphatase, warfarin therapy, frequent drops in blood pressure during hemodialysis, hypercoagulable conditions, corticosteroid and immunosuppressant therapy, calcium-phosphate product of more than 60 mg2/dL2, and use of blood products.5-8 Calcium-phosphate product is the most sensitive risk factor in the diagnosis of calciphylaxis, and small vessel calcification.5,9 BMI is an important predictor of calciphylaxis. Only 5% of hemodialysis patients have a BMI greater than 35 kg/m2 and calciphylaxis develops in 57% of these obese patients.6 Skin trauma, such as that caused by subcutaneous insulin injections in areas vulnerable to calciphylactic lesions, can also precipitate lesion development.6
The current best therapy is prevention. Otherwise, treatment should be guided and modified subjectively. The high mortality and diagnostic difficulty will continue to challenge the physicians and dictate future research in this field.
1. Fine A, Zacharias J. Calciphylaxis is usually non-ulcerating: Risk factors, outcome and therapy. Kidney Int. 2002;61:2210-2217.
2. Selye H. Calciphylaxis. Chicago, Ill: University of Chicago Press; 1962.
3. Budisavljevic MN, Cheek D, Ploth DW. Calciphylaxis in chronic renal failure. J Am Soc Nephrol. 1996;7:978-982.
4. Edelstein CL, Wickham MK, Kirby PA. Systemic calciphylaxis presenting as a painful, proximal myopathy. Postgrad Med J. 1992;68:209-211.
5. Verdalles Guzmán U, de la Cueva P, Verde E, et al. [Calciphylaxis: fatal complication of cardiometabolic syndrome in patients with end stage kidney disease]. Nephrologia. 2008;28:32-36.
6. Parker RW, Mouton CP, Young DW, Espino DV. Early recognition and treatment of calciphylaxis. South Med J. 2003;96:53-55.
7. Bleyer AJ, Choi M, Igwemezie B, et al. A case control study of proximal calciphylaxis. Am J Kidney Dis. 1998;32:376-383.
8. Weenig RH, Sewell LD, Davis MD, et al. Calciphylaxis : natural history, risk factor analysis, and outcome. J Am Acad Dermatol. 200656:569-579.
9. Fischer AH, Morris DJ. Pathogensis of calciphylaxis: study of three cases with literature review. Hum Pathol. 1995;26:1055-1064.