
Two Through Twelve, Something Smells Fishy
 The olfactory nerve is seldom explored during routine physical examination. Take a recent interaction I had with a resident on the delivery of a hemiparesis patient’s cranial nerve status.
The olfactory nerve is seldom explored during routine physical examination. Take a recent interaction I had with a resident on the delivery of a hemiparesis patient’s cranial nerve status.
“Two through 12 normal,” he blurted out, leaving me slightly bewildered and mildly agitated.
I left him feeling the same when I responded, “What happened to cranial nerve 1?”
Perhaps, this spry resident was a fan of the Greek physician, surgeon, and philosopher, Claudius Galen, who was the first to differentiate between nerves, ligaments, and tendons, and viewed the olfactory nerve as part of the brain, not the cranial nerve system.1
Though Vesalius, Eustachius, Falloppio, and other early anatomists differentiated its structure from that of the brain, it was not until Sir Thomas Willis’ classification that the olfactory nerve was considered as the first cranial nerve. Surely, he would be quite pleased to learn that human’s sense of smell—or lack thereof—is under exploration as a predictor of mortality. And, he, as I am, would be quite interested in a study conducted by Pinto et al2 linking hyposmia and anosmia to higher 5-year mortality among older patients.
My initial pass at the study, conducted in 2014, prompted a number of questions:
• Would the results be replicable if more than 5 odors, or different ones were used?
• Would the results be similar if tested among younger patients?
• Knowing that there are acute conditions that cause reversible changes in the sense of smell, does testing that sense only once represent an adequate strategy?
• What would be the reason why many anosmic patients are still alive at the end of the 5-year reassessment?
• Would the authors propose special care for anosmic patients at baseline, to protect them from their omen?
How it Works
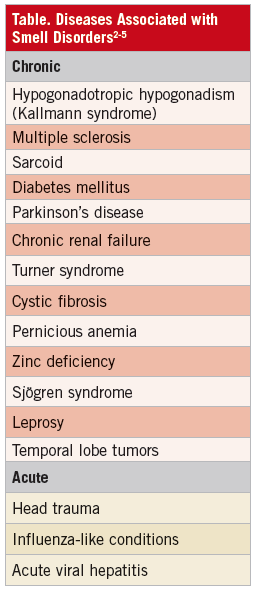
Measuring the exploration of the olfactory nerve’s function consists of letting examinees sniff nonirritating substances, such as cloves, cinnamon, mint, or coffee beans, with their eyes closed, 1 nostril at a time. Although a standard is not clearly defined, it is expected to find people that smell more than others (hyperosmia), somewhat less (hyposmia), or not at all (anosmia).3 These changes can be acute—many times reversible—or chronic. Some of the ailments associated with hyposmia or anosmia are presented in the Table. It is important to acknowledge that the ability to detect a smell is more relevant than identifying the substance.4
The Science of Smell
Pinto et al’s study took several conditions into consideration: nutritional factors, mental health, tobacco or alcohol abuse, and frailty.6 The authors tested the sense of smell using 5 target odors: rose, leather, orange, fish, and peppermint. Participants were asked to identify the odors by pointing at pictures describing the substances.
In this study, anosmia increased the odds of 5-year mortality 4 times over normosmic patients, even if they had comorbidities (ie, chronic obstructive pulmonary disease, cancer, heart attack, stroke, diabetes, or heart failure). Though hypothesized by the authors, the mechanism that linked mortality with smell dysfunction was not identified. The researchers had more than 3000 people (age 57-85) do their best to identify each odor. The team then kept track of these people’s fates over the ensuing half decade.
The important takeaway here is that doctors should pay attention to patients’ senses of smell as an indicator of overall health.
Previous studies found that smell dysfunction in younger patients can predict future neurodegenerative disease7 and patients with Parkinson’s disease have a dose-dependent increased mortality as they accumulate selective anosmia to up to 12 substances.8
Despite its flaws, the study shines the spotlight on a nerve that, when failing, is potentially 1 of the strongest predictors of impending mortality. It is both a fascinating and valuable discovery.
Back to rounds and Pinto’s study, which after subsequent reads, left me wondering if the olfactory nerve will make its way back to the neurologic exam now that it has been elevated to a matter of “life and death.”
Gabriel Aisenberg, MD, is an assistant professor of medicine at the University of Texas Houston Health Science Center and director of general medicine at Lyndon Baines Johnson Hospital, both in Houston, TX.
REFERENCES:
1.Davis MC, Griessenauer CJ, Bosmia AN, et al. The naming of the cranial nerves: a historical review. Clin Anat. 2014;27(1):14-19.
2.Pinto JM, Wroblewski KE, Kern DW, et al. Olfactory dysfunction predicts 5-year mortality in older patients. PLOS One. 2014;9(9):e107541.
3.Walker HK. Cranial nerve I: the olfactory nerve. In: Walker HK, Hall WD, Hurst JW. Clinical Methods—The History, Physical and Laboratory Examinations. 3rd ed. Boston, MA: Butterworth-Heinemann; 1990.
4.Orient JM. Sapira’s Art and Science of Bedside Diagnosis. 3rd ed. New York, NY: Lippincott, Williams & Wilkin; 2009.
5.Garcia-Gonzalez D, Murcia-Belmonte V, Clemente D, De Castro F. Olfactory system and demyelination. Anat Rec. 2013;296(9):1424-1434.
6.Schiffman SS. Taste and smell in disease. N Eng J Med. 1983;309(17):1062-1063.
7.Hüttenbrink KB, Hummel T, Berg D, et al. Olfactory dysfunction: common in later life and early warning of neurodegenerative disease. Dtsch Arztebl Int. 2013;110(1-2):1-7.
8.Wilson RS, Yu L, Bennett DA. Odor identification and mortality in old age. Chem Senses. 2011;36(1):63-67.