
Tethered Cord and Myelolipoma in a Vestigial Tail
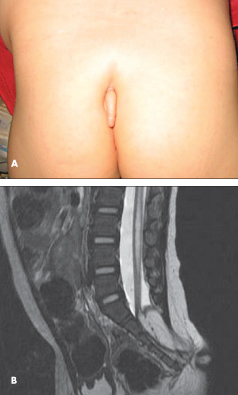 A 17-month-old girl recently adopted from China was brought for evaluation. She was noted to have a 2.5-cm appendage protruding from the sacrum (A). The mass was soft, with no bones or pain on palpation and no swelling or erythema. Examination was remarkable for a left arm that ended mid-forearm, consistent with amniotic banding. Physical findings were otherwise normal, with no noted neurological deficits.
A 17-month-old girl recently adopted from China was brought for evaluation. She was noted to have a 2.5-cm appendage protruding from the sacrum (A). The mass was soft, with no bones or pain on palpation and no swelling or erythema. Examination was remarkable for a left arm that ended mid-forearm, consistent with amniotic banding. Physical findings were otherwise normal, with no noted neurological deficits.
MRI scans of the lumbar spine with and without contrast showed sacral dysraphism from S2 through S5, a lipomyelocele with a tethered cord and a conus ending at S2, and a lipoma that extended through the dysraphic segments into the subarachnoid space encompassing the appendage (B). She also had a syrinx from the T12-L1 interspace to the L5-S1 interspace.
She underwent L5-S2 laminectomy and untethering of the spinal cord as part of removal of the dorsal appendage. She tolerated the procedure well and had good anal sphincter tone as well as good lower extremity tone after the surgery. To date, she is growing well and has normal neurological function.
The human tail is a rare condition (with about 70 cases reported) and is typically classified into 2 categories: a true (vestigial) tail, which contains bone, muscle, nervous tissue, fat, and vascular structures; and a pseudotail, which can have normal and abnormal tissue. Either can be associated with anomalies, such as myelomeningocele, meningocele, or lipoma.1 A fetal tail is normally present from the fourth to eighth week of gestation.2 If it fails to regress, then a vestigial tail will remain.
Human tails have been associated with multiple other anomalies in caudal regression syndrome,3 as part of a VATER (vertebral anomalies, anal stenosis, tracheoesophageal fistula, and radial defects) sequence,4 and in Crouzon syndrome.5 However, these are extremely rare, and no clear association exists for a single syndrome. Multiple studies have looked at caudal appendages; most show that about 50% represent spinal dysraphism, of which a large proportion includes conditions such as meningocele, spina bifida occulta, tethered cord, and/or lipomyelomeningocele.6,7 Thus, in the case of a human tail, presurgical screening, specifically with MRI imaging, to look for neural elements is important.