
Solitary Osteochondroma
Authors:
Joshua Rollins, BS; Adeet Amin, BS; and Lynnette Mazur, MD, MPH
McGovern Medical School at the University of Texas Health Science Center at Houston
Citation:
Rollins J, Amin A, Mazur L. Solitary osteochondroma. Consultant. 2018;58(5):e177.
An 11-year-old girl presented to a clinic with a 3-year history of a mass on the medial aspect of her right knee (Figure 1). The mass was enlarging and becoming more painful, and it particularly had become painful with ambulation. She had no numbness, tingling, or weakness. Radiography revealed a sessile mass measuring 6.0 × 1.6 cm along the medial distal femoral metadiaphysis (Figure 2).


In an unrelated case, a 12-year-old boy presented to the same clinic with a 6-month history of a mass on the lateral aspect of his left leg (Figure 3). He had no pain, numbness, or weakness. Radiography showed a 2.0 × 2.0-cm mass on the lateral aspect of the left fibula (Figure 4).


Because both patients’ radiographs showed sessile ossified lesions with cartilaginous caps that were continuous with the bony cortex, both patients received a diagnosis of osteochondroma.
NEXT: Discussion
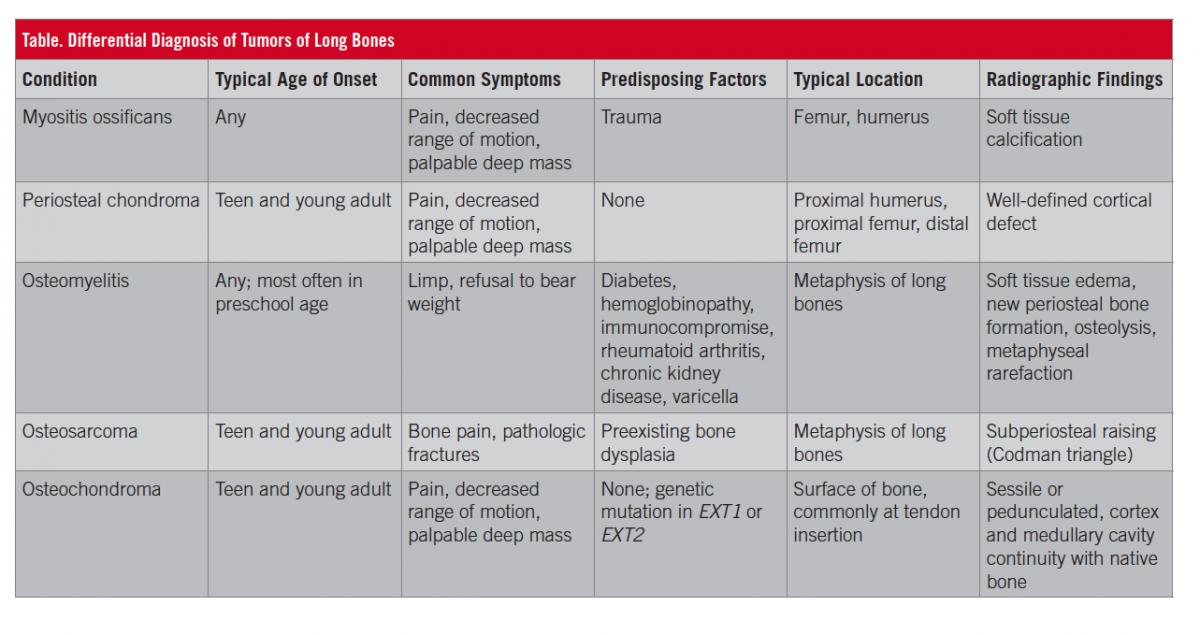
Discussion. Solitary osteochondromas or exostoses are benign cartilage-producing tumors that form at the metaphysis of long bones. As ossified projections with cartilaginous caps, they are distinguished from other masses (Table) by their continuity with the bony cortex, and they may be pedunculated or sessile. Solitary osteochondromas are the most common benign bone tumor and usually occur sporadically. They most often present during the second decade of life and rarely grow beyond the time of skeletal maturity.1
Multiple osteochondromas, also known as osteochondromatosis or multiple hereditary exostoses, are rare. They are an autosomal dominant disorder caused by a mutation in EXT1 or EXT2.2 The mutations may be sporadic, so a negative family history of multiple osteochondromas does not rule out the diagnosis.2
Unlike persons with solitary osteochondromas, which typically present in the second decade of life, persons with osteochondromatosis develop osteochondromas in the first decade of life. Malignant transformation to chondrosarcoma occurs in up to 5% of cases.3 Magnetic resonance imaging (MRI) or computed tomography (CT) may be used to distinguish benign lesions from malignant lesions. Malignant lesions have a thicker cartilage cap. Using 2 cm of cartilage cap thickness as a cutoff for identifying malignant tumors, MRI has 100% sensitivity and 98% specificity, and CT has 100% sensitivity and 95% specificity.3
Osteochondromas are often asymptomatic. Pain is the most common symptom and results from irritation to muscles, tendons, and/or ligaments. In some cases, osteochondromas compress blood vessels or nerves and lead to vascular obstruction or nerve damage. Previously asymptomatic patients tend to develop more symptoms with age, in association with increased participation in contact or impact sports as well as increasing muscle mass and weight.
Lesions in symptomatic patients or in patients with suspicion of malignant transformation are resected. Resection also can be performed for cosmetic reasons.4 Resections can be done by open excision or endoscopically.5 Limited data are available on the recurrence rate after resection but, it appears to be low.6
Outcome of the cases. Both patients were reassured of the benign nature of their lesion and were advised to return if the lesion continued to grow or if symptoms of nerve impingement or vascular obstruction develop.
REFERENCES:
- Yildiz C, Erler K, Atesalp AS, Basbozkurt M. Benign bone tumors in children. Curr Opin Pediatr. 2003;15(1):58-67.
- Mărginean CO, Meliţ LE, Mărginean MO. Daughter and mother diagnosed with hereditary multiple exostoses: a case report and a review of the literature. Medicine (Baltimore). 2017;96(1):e5824.
- Bernard SA, Murphey MD, Flemming DJ, Kransdorf MJ. Improved differentiation of benign osteochondromas from secondary chondrosarcomas with standardized measurement of cartilage cap at CT and MR imaging. Radiology. 2010;255(3):857-865.
- Biermann JS. Common benign lesions of bone in children and adolescents. J Pediatr Orthop. 2002;22(2):268-273.
- Ayerza MA, Abalo E, Aponte-Tinao L, Muscolo DL. Endoscopic resection of symptomatic osteochondroma of the distal femur. Clin Orthop Relat Res. 2007;459:150-153.
- Ng C, Bibiano L, Grech S, Magazinovic B. Antecubital fossa solitary osteochondroma with associated bicipitoradial bursitis. Case Rep Orthop. 2015;2015:560372.