
Pyoderma Gangrenosum
Jordan Burlen, BS, Nicholas Horen, MD, Anu Garg, MD, Jana Meisler, BSN, RN, CWS, CWOCN, CFCN, and Basil E. Akpunonu, MD
University of Toledo College of Medicine, Toledo, Ohio
A 47-year-old woman with history of sarcoidosis was being treated in a long-term acute facility for multiple ulcers that are not responding to multiple antibiotics, wound dressings, and chemical and surgical debridement. She described the lesions as being extremely painful; consequently, she is on high-dose oral and intravenous (IV) narcotics.
History. She had sustained soft tissue injuries to both hips and thighs 3 months earlier while transferring to a wheelchair. The current lesions had started with ecchymosis and subsequently had led to superficial and deep ulcerations. Her past medical history was significant for sarcoidosis (diagnosed by way of scalene node biopsy 4 years earlier), mild hyperglycemia, hypertension, obstructive sleep apnea, and chronic swelling in both lower extremities. She had been admitted to the hospital on 3 occasions for wound care and surgical debridement and had been on various IV antibiotics, including ertapenem and vancomycin. In addition to frequent wound dressing changes, she had had 3 surgical debridements that did not promote healing or cure but that had caused more pain and further expansion of the lesions.
Physical examination. The patient was a bedridden, obese woman weighing 147 kg who was in extreme pain upon movement, positioning, and dressing changes. Vital signs were unremarkable except for significant increases in blood pressure and heart rate related to poor pain control. The lungs were clear, and she had no lymphadenopathy. Although the heart sounds were not distinct, no murmurs or gallops were appreciated. No hepatosplenomegaly was noted.

She had 4 discrete lesions on the hip and thighs, corresponding to the areas of the prior trauma and measuring from 11.3 x 18 x 1.2 cm to 18 x 13.5 x 5 cm (Figure 1). The edges were ill-defined and irregular, had a bluish-purplish hue, and were painful to the touch; deep ulcers were present with exposed subcutaneous fat in various stages of necrosis.
Diagnostic tests. At various points, the patient had elevated white blood cell counts, with a predominance of neutrophils. Her liver panel results showed a low albumin level of 2.4 g/dL (reference range, 3.5-5.0 g/dL) and a low total serum protein level of 6.0 mg/dL (reference range, 6.5-8.0 mg/dL). The erythrocyte sedimentation rate was elevated at 112 mm/h, and the angiotensin-converting enzyme level was normal at 20 U/L (reference range, 8-52 U/L). Histologically, the debrided and skin biopsies showed cutaneous ulceration, gangrenous necrosis, and deep fat necrosis with sheets of neutrophils.
A diagnosis of pyoderma gangrenosum was suspected, given the history of trauma preceding the lesions, the unresponsiveness to antibiotics and surgical debridement, and the severe pain that was out of proportion to what may be expected of similar lesions.
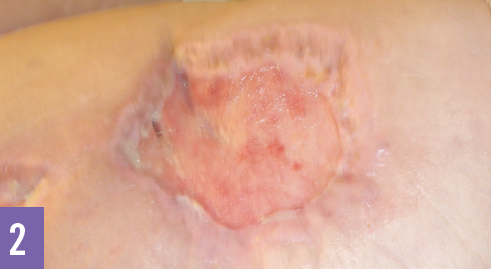
Outcome of the case. The patient was started on a regimen of IV methylprednisolone, 1 g daily for 3 days, leading to relief of pain within 24 to 36 hours. She was maintained on prednisone, 60 mg for 2 months, and continued to show progressive improvement with almost total healing of the lesion within 4 months (Figure 2).
Discussion. Pyoderma gangrenosum is a rarely encountered, painful, cutaneous ulceration of unknown etiology. It often is misdiagnosed and is thought to be caused by immune system dysfunction. The disease incidence is estimated at 3 to 10 cases per million per year, and it can be found in patients of any age, but is seen most commonly in middle-aged women.1
Pyoderma gangrenosum is classified into typical and atypical forms. The typical form most often occurs on the lower extremities and tends to have deeper penetration. The atypical form tends to arise on the upper extremities and is more superficial.2 The disease is further subclassified by appearance as ulcerative, pustular, bullous, or vegetative types. The ulcerative form, the most common, presents with necrotic and mucopurulent painful ulcer with a pathognomonic blue, serpiginous border. A unifying characteristic of pyoderma gangrenosum lesions is the association with pathergy.1,3 Pathergy is a phenomenon seen with progression and extension of the lesions and ulcers when they are traumatized even minimally and by surgical debridement. For this reason, surgical debridement should be avoided in most suspected cases.2,3
Pyoderma gangrenosum has been associated with underlying systemic diseases, inflammatory bowel disease, various arthritic diseases, immunologic deficiencies, and hematologic malignancies, but cases of pyoderma gangrenosum associated with sarcoidosis are exceedingly rare. Pyoderma gangrenosum and sarcoidosis share a presentation of abnormal chemotaxis, phagocytosis, cutaneous anergy, T cell abnormalities, and pathergy.4-6 Immunosuppressive therapy with high-dose IV corticosteroids is the most commonly used initial treatment, followed by a decreasing dose of corticosteroids, which often is combined with other immunosuppressants, immunomodulators (eg, cyclosporine, mycophenolate mofetil, tacrolimus, infliximab), and plasmapheresis, depending on the responses.7
The prognosis is good for most patients who take extra precautions to prevent further trauma.8 Residual scarring is a common finding, and recurrence is common.9
We suggest that a diagnosis of pyoderma gangrenosum be considered in cases of recalcitrant purulent lesions that develop and spread suddenly, worsen with surgical debridement, and are associated with disproportionate pain. Treatment with immunosuppressive agents usually is effective.
References:
- Ruocco E, Sangiuliano S, Gravina AG, Miranda A, Nicoletti G. Pyoderma gangrenosum: an updated review. J Eur Acad Dermatol Venereol. 2009; 23(9):1008-1017.
- Bennett ML, Jackson JM, Jorizzo JL, Fleischer AB Jr, White WL, Callen JP. Pyoderma gangrenosum: a comparison of typical and atypical forms with an emphasis on time to remission: case review of 86 patients from 2 institutions. Medicine. 2000;79(1):37-46.
- Armstrong PM, Ilyas I, Pandey R, Berendt AR, Conlon CP, Simpson AH. Pyoderma gangrenosum: a diagnosis not to be missed. J Bone Joint Surg Br. 1999;81(5):893-894.
- Bhat RM, Nandakishore B, Sequeira FF, et al. Pyoderma gangrenosum: an Indian perspective. Clin Exp Dermatol. 2011; 36(3):242-247.
- Powell FC, Schroeter AL, Su WPD, Perry HO. Pyoderma gangrenosum and sarcoidosis. Arch Dermatol. 1984;120(7):959-960.
- English JC III, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol. 2001;44(5):725-743.
- Chow RKP, Ho VC. Treatment of pyoderma gangrenosum. J Am Acad Dermatol. 1996;34(6):1047-1060.
- DeFilippis EM, Feldman SR, Huang WW. The genetics of pyoderma gangrenosum and implications for treatment: a systematic review. Br J Dermatol. 2015;172(6):1487-1497.
- Jacob SE, Weisman RS, Kerdel FA. Pyoderma gangrenosum—rebel without a cure? Int J Dermatol. 2008;47(2):192-194.