
Probiotics: What Clinicians Need to Know
ABSTRACT: While probiotics remains a big business in the United States and across the world, the use of live “friendly” organisms to decrease bad bacteria in the colon remains in debate. This article reviews how probiotics function in the human gut, provides a synopsis on the current evidence-based research, and gives primary care practitioners an overview of appropriate recommendations for specific probiotic products.
Probiotics are live bacteria, primarily found in foods, that produce a health effect in the host.1 The use of probiotics has a lengthy history. At the beginning of the 20th century, Bulgarian peasants were thought to live long and fit lives due to their consumption of fermented milk containing lactic acid bacteria.1,2 During a World War I outbreak of shigellosis, a new strain of Eschericia coli was discovered in the stool of a soldier who was exposed to shigella, but did not develop the diarrheal illness. That strain was later used to treat intestinal infections with success.1
Probiotics are a lucrative business in the United States—43% of Americans purchase these foods and supplements, spending $1.2 billion annually.1 The worldwide demand for probiotic products is expected to exceed $32.6 billion in 2014.3
____________________________________________________________________________________________________________________________________________________________________
RELATED CONTENT
Probiotics Could Curb Blood Pressure
Are Probiotics the Secret to Healthier Skin?
____________________________________________________________________________________________________________________________________________________________________
Understanding Probiotics
The word probiotics is derived from the Greek term, biotikos, which translates to for life. The clinical benefit of probiotics in the treatment of multiple digestive illnesses can be traced back to the 1990s.4 Probiotics have a 3-fold role: prevent the growth of bad bacteria by competing for space and nutrients, lower intestinal pH, and increase the production of mucin which acts as a blockade. This blocking action subsequently decreases the permeability of the gut and prevents pathogenic bacteria from adhering to the intestinal wall.5
The human GI tract is populated with a hefty assortment of microbes, estimated at 10 times the total number of cells in the human body. The intestinal flora is often referred to as microbiota.1 The microbiota inside and outside the body amid their genomes are known as a microbiome.6
Microbiome begins development shortly after birth, at which time the newborn’s microbiota mirrors that of the mother’s skin (cesarean section) or birth canal (vaginal delivery). Within 1 to 2 years, the youngster’s microbiome is similar to that of an adult. The microbiome continues to evolve under the influence of gender, geography, health status, diet, genetics, and early microbial exposure.1,6
Role of Antibiotics
Researchers have documented that the administration of antibiotics can have an unintentional outcome on the microbiome. Antibiotics are considered one of the most prescribed drugs in the world; Taggart and Bergstrom estimated that British children have been prescribed an average of 10 to 20 courses of antibiotics by the time they reach their 18th birthday.6 These researchers also reported a 5-day supply of ciprofloxacin changed the intestinal microbial environment for 1 month post-antibiotic treatment, while the combination of clarithromycin and metrodiazole plus omeprazole saw no recovery in the gut flora to pre-antibiotic status even after 4 years. 6
Clostridium difficile infection (CDI) is likely the most infamous antibiotic consequence on the human microbiome. CDI is thought to result from demolition of the GI flora during antibiotic treatment, which consequently lowers resistance to pathogens such as C difficile. CDI varies in its effects on the human host—ranging from asymptomatic diseases to colitis and even death.
An appalling $3.2 billion is spent annually in caring for patients who develop CDI. However, research consistently documents that probiotics ingested during the course of antibiotic treatment are useful in counteracting the changes in the normal gut microbiota, thereby reducing the risk of CDI.7-9
Probiotics vs Illness
Probiotics can help treat a multitude of other illnesses:
• Diarrhea. One study found that individuals who consumed probiotics for infectious diarrhea were sicker for a shorter period of time. Another study showed that persons taking probiotics while on antibiotic therapy reduced their risk of antibiotic-associated diarrhea.1 In fact, the American Academy of Pediatrics supports probiotics for the treatment of viral gastroenteritis and antibiotic-associated diarrhea in children.6
• Atopic disease. A meta-analysis of probiotic administration in early life also appears to have measurable impact on atopic disease.10 In a study of 40,000 children where parents reported atopic eczema, rhinoconjunctivitis, and asthma in their offspring, researchers noted that probiotic supplementation by the mother during pregnancy and continued consumption by the infant appreciably lowered incidence of atopic eczema and rhinoconjunctivitis; no reduction in asthma was seen.11
Foolad and Armstrong reviewed 13 studies where 61.5% of participants indicated that ingesting probiotics contributed to better prevention of atopic dermatitis.12 Five of those studies specifically identified Lactobacillus rhamnosus GG as effective both in preventing and diminishing the severity of atopic dermatitis.12
Similarly, investigators documented a considerable improvement in adult atopic dermatitis when strains of L. salivarius and Bifidibacterium breve were used conjointly.13
• GI issues. Probiotics were also found to reduce crying time in breastfed babies with colic.14 Investigators reported a reduction in abdominal pain after children who were diagnosed with irritable bowel syndrome (IBS) ate probiotic foods15 and similar symptom relief in adult IBS patients.16 A meta-analysis investigating the prevention of travelers’ diarrhea (TD) indicated that probiotics significantly eliminated symptoms.9
• Triglycerides and high-density lipoprotein (HDL). In one study, intensive care patients were randomized to receive a placebo or probiotic. Investigators noted reduced levels of triglycerides and increased HDL levels in participants receiving the probiotic; no change in total cholesterol or low-density lipoprotein cholesterol could be appreciated.17
• Radiation. Patients treated with pelvic radiation and probiotics concurrently noted a reduction in diarrhea post-intervention.18
• Dental cavities. Children who were given probiotics at a daycare center reported significantly lower rates of dental cavities after consuming probiotics.8
Selecting the Right Probiotic
When evaluated as a single product, existing research confirms specific probiotic strains may treat or avert some illnesses. The conundrum of probiotics is that there is no fundamental equivalency between the hundreds of strains that exist. Different strains of even the same species can be disparate in actions and benefits.
A probiotic strain is defined by its genus (eg, Lactobacillus), species (eg, plantarum), and the strain designation (a combination of letters and numbers, such as 299V). Seldom do the claims for health benefits on the product packaging connect the precise probiotic strain inside to a particular medical condition.
In the literature and advertised media, probiotics are frequently hailed as supplements that can fortify the immune system or replenish the intestine with beneficial bacteria before, during, or after an illness. Probiotics are found in yogurt, some cheeses, sauerkraut, buttermilk, and over-the-counter dietary supplements that are easily accessed by both patients and families. In addition, there are hundreds of probiotics in the marketplace, making it tough, if not impossible, for the consumer to choose the best item for consumption. Consequently, patients are liable to select an unsuitable or useless product.
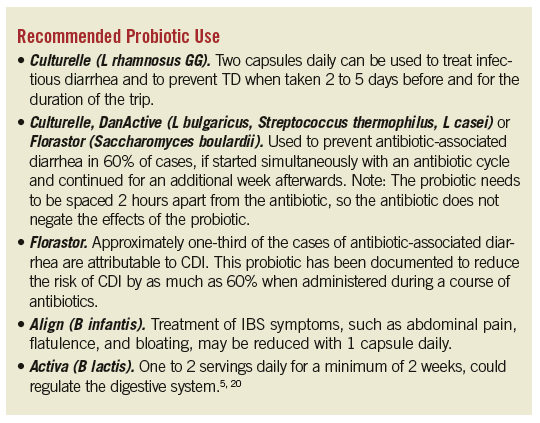
Clinicians should advocate a product based on sound evidence of efficacy when consulting with patients regarding probiotics. Advise patients to choose a recognized manufacturer with packaging that includes the strain, how many live active cultures are present per serving, the expiration date, how much and how often the product should be consumed, the health benefits expected, and how to find out more information (see Recommended Probiotic Use). Remind patients that dairy products generally have a short shelf life and usually require refrigeration to ensure a viable product. Finally, stress that probiotics may only provide a temporary benefit and will likely require continued ingestion to maintain the health enhancement.
Although probiotics by and large are considered safe in healthy human hosts and have been part of human dietary intake for centuries, there is a hypothetical risk for infection in immunocompromised patients.1,21 Also, it is important to recognize most normal healthy people do not require probiotics to maintain a robust digestive system. The decision to propose probiotics as an optional or adjunct remedy must be made in light of the patient’s individual condition and wishes. Make evidence-based decisions when selecting precise probiotics to treat specific medical conditions.
The challenge for future investigations is to increase the numbers of study participants and test more strains on a variety of particular illnesses in order to best appraise the health benefit of probiotics. Research should also examine the role of probiotics as part of the healthy diet rather than a supplement.
References:
1.Piascik M, Sanders ME. Probiotic supplementation: what nurse practitioners need to know to recommend safe and effective formulations.
www.powerpak.com/course/preamble/108730. Accessed November 2014.
2.Gordon S. Elie Metchnikoff: father of natural immunity. Eur J Immunol. 2008;38(12):3257-3264.
3.Brody J. Probiotic logic vs gut feelings. The New York Times. July 21, 2014. http://well.blogs.nytimes.com/2014/07/21/probiotic-logic-vs-gut-feelings/?_r=0. Accessed November 5, 2014.
4.Health benefits of taking probiotics. Harvard Medical School Family Health Guide. 2005. www.health.harvard.edu/fhg/updates/update0905c.shtml. Accessed November 2014.
5.Therapeutic Research Center. Probiotics: an update. 2009. http://pharmacistsletter.therapeuticresearch.com/cat3557-Natural-Medicines-Probiotics/Browse.aspx?s=PL. Accessed November 2014.
6.Taggart H, Bergstrom L. An overview of the microbiome and the effects of antibiotics. J Nurse Pract. 2014;10(7):445-450.
7.Goldenberg JZ, Ma S, Saxton JD, et al. The prevention of Clostridium difficile-associated diarrhea in adults and children. Cochrane Database Syst Rev. 2013;5:CD006095.
8.Goldin BR, Gorbach SL. Clinical indications for probiotics: an overview. Clin Infect Dis. 2008;46(Suppl 2):S96-S100.
9.McFarland LV. Meta-analysis of probiotics for the prevention of traveler’s diarrhea. Travel Med Infect Dis. 2007;5(2):97-105.
10.Elazab N, Mendy A, Gasana J, et al. Probiotic administration in early life, atopy, and asthma: a meta-analysis of clinical trials. Pediatrics. 2013;
132(3):e666-676.
11.Bertelsen RJ, Brantsaeter AL, Magnus MC, et al. Probiotic milk consumption in pregnancy and infancy and subsequent childhood allergic diseases. J Allergy Clin Immunol. 2014;133(1):165-171.
12.Foolad N, Armstrong AW. Prebiotics and probiotics: the prevention and reduction in severity of atopic dermatitis in children. Benef Microbes. 2014;5(2):
151-160.
13.Iemoli E, Trabattoni D, Parisotto S, et al. Probiotics reduce gut microbial translocation and improve adult atopic dermatitis. J Clin Gastroenterol. 2012;
46 Suppl:S33-S40.
14.Sung V, Collett S, de Gooyer T, et al. Probiotics to prevent or treat excessive infant crying: systematic review and meta-analysis. JAMA Pediatr. 2013;
167(12):1150-1157.
15.Korterink JJ, Ockeloen L, Benninga MA, et al. Probiotics for childhood functional gastrointestinal disorders: a systematic review and meta-analysis. Acta Paediatr. 2014;103(4):365-372.
16.Ducrotte P, Sawant P, Jayanthi V. Clinical trial: Lactobacillus plantarum 299v (DSM9843) improves symptoms of irritable bowel syndrome. World J Gastroentrol. 2012;18(30):4012-4018.
17.Sanaie S, Ebrahimi-Mameghani M, Mahmoodpoor A, et al. Effects of a probiotic preparation (VSL#3) on cardiovascular risk parameters in critically-ill patients. J Cardiovasc Thorac Res. 2013;5(2):67-70.
18.Demers M, Dagnault A, Desjardins J. A randomized double blind controlled trial: impact of probiotics on diarrhea in patients treated with pelvic radiation. Clin Nutr. 2014;33(5):761-767.
19.International Scientific Association for Probiotics and Prebiotics. The p’s and q’s of probiotics: a consumer’s guide for making smart choices.
www.bifantis.com/pdf/Ps_and_Qs_of_probiotics.pdf. Accessed November 2014.
20.Probiotics self-study course. Pharmacist Letter. 2013;13(103):130103.
21.Therapeutic Research Center. Comparison of common probiotic products. 2012. http://pharmacistsletter.therapeuticresearch.com/pl/Browse.aspx?cs=&s=PL&pt=2&fpt=31&dd=250908&pb=PL&cat=5718&segment=1771. Accessed November 2014
Candace Sandal, DNP, MBA, APRN, COHN-S is the health services manager for The Dow Chemical Company in Newark, DE, and an associate professor at Wilmington University in Wilmington, DE.