
Pott Puffy Tumor
Authors:
Elizabeth A. Chu, BA, MS
Touro College of Osteopathic Medicine, New York, New York
Sarika Sunku, MD
Nyack Hospital, Nyack, New York
Citation:
Chu EA, Sunku S. Pott puffy tumor. Consultant. 2018;58(4):158, 160.
A 16-year-old boy presented to our emergency department (ED) with rhinorrhea, facial pain, and forehead swelling that had begun that day, along with significant headaches following an upper respiratory tract infection 2 weeks prior. He initially had attributed the headaches to trauma from playing football, but the headaches had continued to worsen.
History. He had been taking over-the-counter ibuprofen and an acetaminophen, aspirin, and caffeine preparation, which had led to some headache relief. He also had been taking amoxicillin, prescribed by his pediatrician for presumed sinusitis 4 days prior to presenting in the ED, with no improvement in symptoms.
At the ED visit, the patient denied nausea, fever, stiff neck, photophobia, visual symptoms, tearing, and toothache or recent dental infection. A noncontrast computed tomography (CT) scan of the sinuses revealed opacification of the bilateral frontal sinuses with hyperdense secretions of the right frontal sinus, findings consistent with acute frontal sinusitis. The patient was discharged from the ED on a regimen of amoxicillin-clavulanate.
The patient returned to the ED the next day with worsening headaches.
Physical examination. At this ED visit, evaluation of the head revealed significant swelling and tenderness of the frontal area extending to the glabella. No induration or erythema was noted. The auditory canals and tympanic membranes appeared normal, with no effusion or inflammation. Nasal examination revealed a midline septum with normal turbinates. Minimal mucoid discharge was noted bilaterally.
Flexible nasal pharyngoscopy was performed by an otorhinolaryngologist and revealed a narrowed right middle meatus with some edema but no purulent discharge. The left middle meatus was patent with minimal edema. The nasopharynx was unremarkable. Physical examination findings of the oral cavity and oropharynx were unremarkable. There was no restriction of extraocular movements. The neck was supple with no adenopathy or thyromegaly.
The patient had an irregular heart rate and arrhythmia consistent with premature atrial contractions. Neurologic examination revealed no abnormalities in the function of cranial nerves II through XII, although the patient was unable to raise his eyebrows as a result of the forehead swelling.
NEXT: Diagnostic Tests
Diagnostic tests. Results of laboratory tests in the ED showed a C-reactive protein (CRP) level of 0.93 mg/dL (reference value, < 0.4 mg/dL) and a white blood cell (WBC) count of 11,800/µL (reference range, 4000-11,500/µL). Results of a manual differential showed 77% segmented neutrophils (reference range, 42%-75%) and 7% lymphocytes (reference range, 20%-51%).
The patient was admitted as an inpatient to the pediatrics floor and started on intravenous (IV) corticosteroids, ceftriaxone, clindamycin, and ibuprofen or ketorolac for pain. Repeated laboratory tests on showed an increase of the CRP level to 1.93 and the WBC count to 14,600/µL.
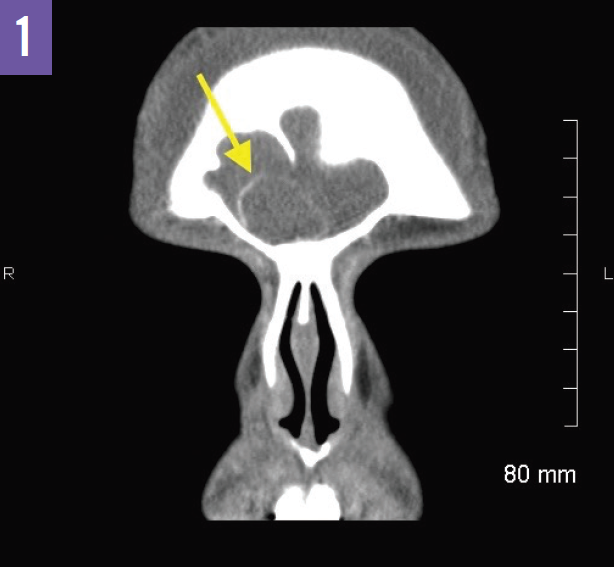
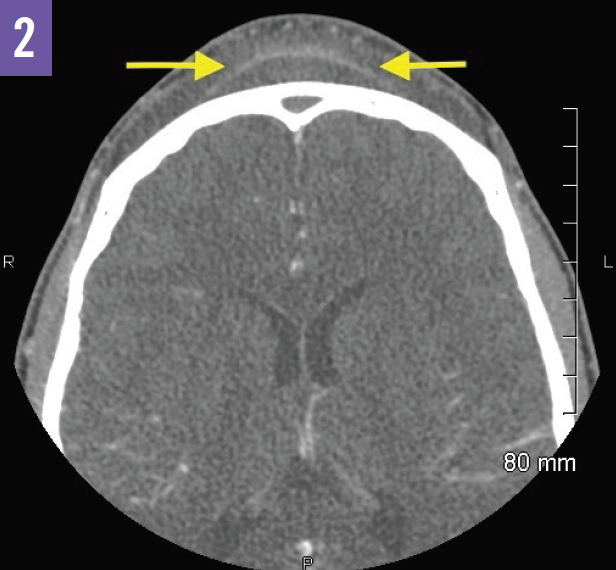
A contrast-enhanced CT of the sinuses performed after admission revealed complete opacification of the frontal sinuses and thinning of the inner table of the right frontal sinus. There was expansion of the bony margins of the right frontal sinus and a well-marginated collection in the right frontal sinus with a thin hyperdense rim (Figure 1). A thin-walled subgaleal collection was noted in the forehead at the midline overlying the outer table of the frontal sinuses (Figure 2). These CT findings were consistent with severe acute sinusitis with spread of infection into the soft tissues of the forehead and nasal bridge, or Pott puffy tumor. While there was no evidence of subdural empyema, a contrast-enhanced magnetic resonance imaging (MRI) scan of the brain was recommended to evaluate for subtle changes such as dural enhancement.
NEXT: Outcome of the Case, Discussion
Outcome of the case. After an otorhinolaryngology consult in our hospital, the patient was transferred to a children’s hospital for drainage of a possible abscess and treatment of Pott puffy tumor. There, antibiotics and fluids were continued, and after evaluation by an otorhinolaryngologist, he underwent uncomplicated right trepanotomy and septoplasty for frontal sinus and abscess drainage. Postoperatively, the patient had a marked reduction in pain and swelling. He continued to receive antibiotics, and the drain was removed by the otorhinolaryngologist. A peripherally inserted central catheter was placed for long-term IV antibiotic therapy. The patient was cleared for discharge after a weeklong stay with close follow-up by otorhinolaryngology, infectious disease, and pediatrics specialists.
Discussion. Pott puffy tumor is a frontal osteomyelitis with associated subperiosteal abscess of the frontal bone.1 It presents with a “puffy,” circumscribed appearance at the anterior table of the frontal bone due to spread of the infection between the periosteum and bone. Common causes of infection include frontal sinus trauma, hematogenous spread of sinusitis, and retrograde thrombophlebitis via the diploic veins.1 However, Pott puffy tumor has also been reported as a complication of insect bites, mastoiditis, and pansinusitis.2
Pott puffy tumor has a predilection for preteen and teenaged boys.1 The frontal sinuses mature to normal adult size at approximately 12 to 13 years of age.3 Additionally, because the vascularity of the diploic veins peaks in adolescence, septic thrombi originating from the frontal sinus can travel along this venous system. These anatomic and developmental considerations explain why Pott puffy tumor tends to be a complication of frontal sinusitis in adolescents.1
Presenting symptoms, in addition to the classic frontal swelling, may include fever, cough, rhinorrhea, and headache.4 Symptoms such as nausea, vomiting, obtundation, pupillary dilation, and aphasia may signal neurologic decompensation due to complications.
The diagnosis is based mainly on presentation. The gold standard diagnostic study is CT of the brain. If CT is insufficient for diagnosis, contrast-enhanced MRI of the brain may help to further evaluate the extent of the infection intracranially and/or detect potential intracranial complications of Pott puffy tumor; these may include subdural or epidural empyemas, brain abscesses, and sinus thromboses.4 MRI is sometimes preferred in the pediatric population so as to avoid exposure to ionizing radiation from CT.
The management of Pott puffy tumor calls for IV antibiotics, analgesia, and surgical intervention if symptoms persist or progress. While endoscopic endonasal treatment has become an option with the advancement of surgical techniques, an external approach should be considered in patients who present with subcutaneous collections.5 IV antibiotic therapy usually continues for 6 to 8 weeks postoperatively.
References:
- Suwan PT, Mogal S, Chaudhary S. Pott’s puffy tumor: an uncommon clinical entity. Case Rep Pediatr. 2012;2012:386104.
- Grewal HS, Dangaych NS, Esposito A. A tumor that is not a tumor but it sure can kill! Am J Case Rep. 2012;13:133-136.
- Blackman SC, Schleiss MR. Forehead swelling caused by Pott’s puffy tumor in a 9-year-old boy with sinusitis. Pediatr Int. 2005;47(6):704-707.
- Stammers D, Juaid AA, Fanella S. Case 2: forehead mass in a teenager. Paediatr Child Health. 2013;18(6):305-306.
- Lauria RA, Laffitte Fernandes F, Brito TP, Pereira PSG, Chone CT. Extensive frontoparietal abscess: complication of frontal sinusitis (Pott’s puffy tumor). Case Rep Otolaryngol. 2014;2014:632464.