
Pneumomediastinum in Children
A 16-year-old boy presented to the pediatric emergency department with a 1-day history of progressively worsening neck and chest pain. He described his neck pain as a squeezing tightness near the sternal notch that intensified with swallowing and coughing. He denied hoarseness, vocal change, shortness of breath, or dyspnea. Interestingly, the patient volunteered that he had participated in a “belching competition” 36 hours before presentation.

Figure 1. A lateral chest radiograph showed the presence of air in the retrosternal and prevertebral spaces of a 16-year-old boy, indicating pneumomediastinum.
On physical examination, the boy’s vital signs were normal and stable. He was in no acute distress and spoke in full sentences. No crepitus or subcutaneous emphysema was appreciated, and the lungs were clear to auscultation, with good air entry bilaterally.
Radiographs (Figures 1 and 2) and computed tomography (CT) scans of the chest and neck were ordered (Figures 3 and 4) and confirmed pneumomediastinum but failed to identify an etiology. Because spontaneous pneumomediastinum is uncommon, the patient was admitted to the pediatric floor for further workup and evaluation. Otolaryngology was consulted.

Figure 2. A cervical radiograph showed the presence of air in the retropharyngeal space.
The otolaryngologist performed flexible fiberoptic nasopharyngolaryngoscopy and discovered a ruptured laryngeal vestibule, which likely had resulted from the excessive belching and likely had caused the pneumomediastinum. The patient’s respiratory status remained stable, and he was discharged home with instructions to avoid forceful belching. He was advised that the pneumomediastinum would resolve spontaneously in a few days.
DISCUSSION
Pneumomediastinum is uncommon in pediatric patients, and its etiology is multifactorial. Spontaneous pneumomediastinum is not associated with chest trauma, lung disease, mechanical ventilation, or other invasive procedures. It is, however, associated with activities that lead to an elevation in alveolar pressure, such as forceful coughing, vomiting, Valsalva maneuvers, playing musical wind instruments, and using inhaled illicit drugs.1 The unique cause of our patient’s pneumomediastinum was a vestibular rupture secondary to belching.
The typical development of pneumomediastinum is described in a sequence of events known as the Macklin effect: alveolar rupture, air dissection along the bronchovascular sheath, and free air reaching the mediastinum.2 The dissection of free air may not be confined to the mediastinum. Because the mediastinum communicates with the spaces of the neck, air that once had been within the mediastinum may dissect through tissue planes, causing pneumopericardium and pneumothorax.3 With a vestibular rupture, air tracks along the retropharyngeal space where it may communicate with the mediastinum.
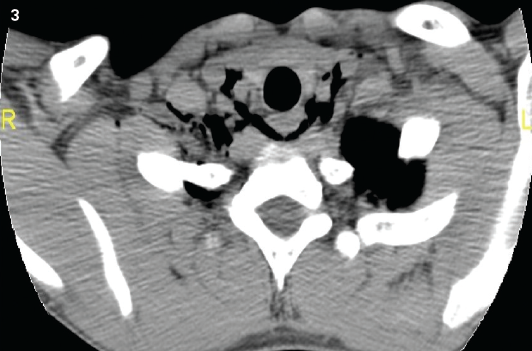
Figure 3. A chest CT scan revealed the presence of air in the paratracheal region.
Our patient likely had a congenital defect in the laryngeal ventricle, which predisposed him to a dehiscence with the increased pressure of belching. The amount of air tracking along the retropharyngeal space was not large enough to produce subcutaneous emphysema.
Chest radiography can reveal air within the mediastinal space and usually is the first step in identification of pneumomediastinum. The typical features of pneumomediastinum on chest radiography are a result of air outlining the anatomic structures in the mediastinum (ie, margins of the heart, retrosternal space, trachea).3 Chest CT can provide additional diagnostic information about the presence of coexisting illness or major injury to the pulmonary and digestive tracts.4 Nevertheless, the etiology of the pneumomediastinum may not be revealed on radiographs or CT scans, and further workup may be needed.
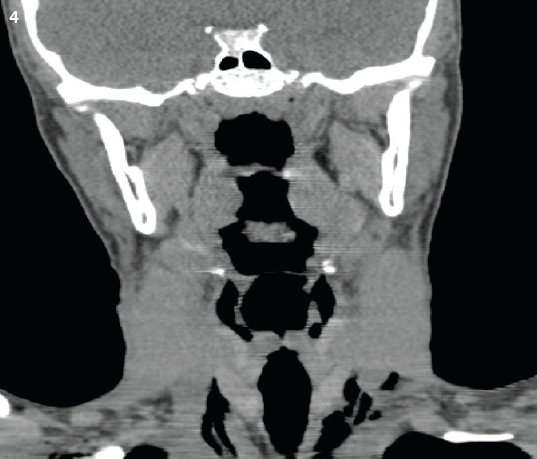
Figure 4. A sagittal CT scan of the neck showed the presence of air in the paratracheal space.
Medical therapy depends on the patient’s clinical status. Management is conservative and typically consists of treating the underlying cause (if identified), rest, analgesics, clinical monitoring, and follow-up. Maneuvers that increase pulmonary pressure should be avoided. Obtaining a thorough history may help identify the cause or contributory factors. Predisposing factors should be identified and controlled to prevent recurrence. Most children with pneumomediastinum are asymptomatic, and the natural course of the condition is spontaneous resolution.5
Listen to a discussion with the author:REFERENCES:
1.Chalumeau M, Le Clainche L, Sayeg N, et al. Spontaneous pneumomediastinum in children. Pediatr Pulmonol. 2001;31(1):67-75.
2.Macklin CC. Pneumothorax with massive collapse from experimental local over-inflation of the lung substance. Can Med Assoc J. 1937;36(4):414-420.
3.Zylak CM, Standen JR, Barnes GR, Zylak CJ. Pneumomediastinum revisited. Radiographics. 2000;20(4):1043-1057.
4.Dissanaike S, Shalhub S, Jurkovich GJ. The evaluation of pneumomediastinum in blunt trauma patients. J Trauma. 2008;65(6):1340-1345.
5.Macia I, Moya J, Ramos R, et al. Spontaneous pneumomediastinum: 41 cases. Eur J Cardiothorac Surg. 2007;31(6):1110-1114.