
Optimizing Post-Resuscitation Care in the Emergency Department: Key Interventions for Reversing the Pathophysiological Manifestations of Post-Resuscitation Syndrome
ABSTRACT: Managing out-of-hospital cardiac arrest continues to be a challenge to healthcare providers. Patient survival rates are low, despite great advances in resuscitation science research and technology. As discussed in part 1 of this article series, published in the February 2015 issue of Consultant, a standardized systems-of-care approach should be applied with the goal of neurologically intact survival. To achieve this goal, optimal in-hospital therapies should begin in the emergency department and center on evidence-based interventions. This article, the second and final installment in the series, focuses on these interventions, reviewing the use of mild therapeutic hypothermia and coronary reperfusion with immediate angiography and percutaneous coronary intervention.
___________________________________________________________________________________________________________________________________________________
Individuals who experience sudden out-of-hospital cardiac arrest (OHCA) require prompt and aggressive treatment that starts in the field and continues through hospital admission. Care of these patients is complex and time-sensitive, necessitating a multidisciplinary approach that accommodates a wide spectrum of patients, from those who arrive to the emergency department (ED) hemodynamically stable and awake to those who are comatose and unstable with a persistent underlying pathology. To ensure optimal outcomes, treatment must focus on reversing the pathophysiological manifestations of post-resuscitation syndrome (PRS), including neurologic injury, myocardial dysfunction, systemic ischemia, and the pathology that precipitated the cardiac arrest. Two interventions are key to addressing these PRS manifestations: mild therapeutic hypothermia (MTH) and coronary reperfusion with immediate angiography and percutaneous coronary intervention (PCI).
MTH is the first and only therapy proven to reverse post-ischemic neurologic injury, and it has forever changed post-
resuscitation care. Multiple major clinical trials and countless case reports have shown this breakthrough therapy to improve neurologically intact survival after OHCA.1-4 However, for the greatest benefits of MTH to be achieved, it must be combined with coronary reperfusion to reverse the underlying arrest pathology. This article provides an overview of these treatments and how to optimize them.
__________________________________________________________________________________________________________________________________________
Related Content
Optimizing Post-Resuscitation Care in the Emergency Department: Addressing Post-Resuscitation Syndrome With a Structured Early Goal-Directed Approach
Trauma Resuscitation of the Elderly Patient
___________________________________________________________________________________________________________________________________________
Mild Therapeutic Hypothermia
PRS involves temperature-dependent processes that cause direct and secondary neuronal injury. When body temperature is rapidly dropped to between 32°C and 34°C for 12 to 24 hours, many of the destructive processes are drastically reduced, enabling the body to mitigate further damage, reinstate self-healing measures, and prevent the massive neurologic injury that typically ensues in the noncooled patient.2
In the medical literature, MTH is often initiated using a 3-phase practical approach. The process begins with the induction phase, where rapid cooling drops the core body temperature to between 32°C and 34°C. Of the 3 phases, this one poses the greatest challenge because of the rapid temperature change; however, the faster the target temperature is reached, the less risk for adverse effects.2 Concern over adverse effects may prevent providers at hospitals without sophisticated cooling equipment from providing MTH; however, the lack of such equipment should not prevent initiation of this therapy. Induction can be rapidly and easily achieved using surface and intravascular methods that are available in any hospital setting. This method starts with administering 2 L (30 mL/kg) of ice-cold isotonic saline intravenously and then instituting surface methods, such as applying cold wet blankets and ice packs to the patient.5
If peripheral and central vascular access were not obtained, the intraosseous (IO) route can be considered; however, the intravenous (IV) route is considered to be far superior for reaching target temperature than IO infusion.6 When comparing the use of more sophisticated commercial water-flow systems and endovascular methods with the use of cold wet blankets and ice packs, all were equally effective at reaching target temperatures, but the sophisticated methods were more effective at maintaining target temperatures.7
The second phase of MTH is the maintenance phase, where maintaining the targeted temperature is the key. Here, fluctuations in core temperature must be minimized; a goal best attained through invasive temperature measurement using esophageal, rectal, or bladder probes. While all 3 theoretically measure an accurate core temperature, several reports suggest that esophageal probes offer the most accurate measurement.8,9 Along with solid temperature tracking methods, consistent cooling tactics must be used. Ice packs coupled with IV saline may be helpful at induction, and although maintaining target temperatures is feasible with these methods,5 they will likely be more labor-intensive for the nursing staff.7,10 Advanced endovascular catheter systems provide real-time feedback, can maintain a tight temperature range more easily than less sophisticated methods, and will also allow controlled rewarming.7 Antibiotic prophylaxis should be considered during this phase, as should the prevention of decubitus ulcers.2
The third and final phase of MTH is the rewarming phase, which takes place after 24 hours at the target temperature. Rewarming should occur slowly at a rate of 0.2°C to 0.5°C per hour, as rapid rewarming can reinitiate the destructive processes that were initially prevented with MTH.2 Prognostication regarding neurologic outcome cannot take place until at least 72 hours after rewarming has occurred. This 3-day period is crucial for sedative clearance, enabling an accurate neurological examination to provide prognostic details.11 During this time, if normothermia is attained, every effort must be made to maintain this temperature; this so-called “controlled normothermia” provides gentle cooling to maintain a body temperature of 37°C and prevent pyrexia.10
For MTH to maximize its advantages, several important points should be remembered. First, the aforementioned sequence of treatment is safe to apply to all comatose and intubated survivors of OHCA, whether stable or critically unstable.12 While patients experiencing ventricular fibrillation/polymorphic ventricular tachycardia (VF/pVT) arrests have clearly shown the best outcomes with MTH, those patients with non-VF/pVT presenting rhythms should still be considered for this therapy. Second, MTH should not be delayed after return of spontaneous circulation (ROSC) and should be initiated by emergency medical services (EMS) or ED staff promptly on arrival to the ED. Between 6 to 12 hours after ROSC is the period of utmost importance for the initiation of MTH, after which the damage may be irreversible.10 Finally, MTH should be included in a standardized treatment strategy, provided simultaneously with the hemodynamic stabilizing effects of early goal-directed therapy (EGDT), and be continued during PCI.8,12-18
 Mild Therapeutic Hypothermia Caveats
Mild Therapeutic Hypothermia Caveats
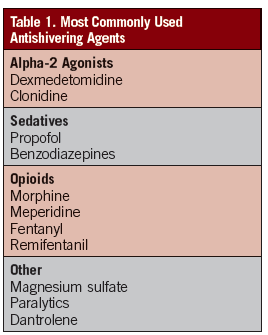
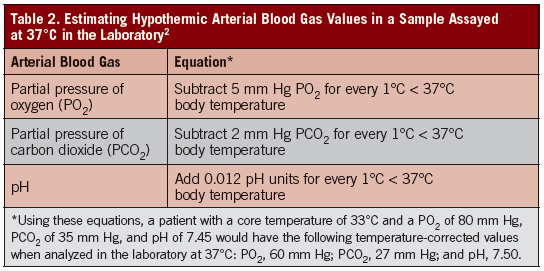
When applying the principals of EGDT during the induction phase of MTH, physicians need to be vigilant regarding several physiologic side effects that have the propensity to affect therapy goals.2 Rapid reduction of core temperature decreases the metabolic rate by ±8% per 1°C drop in temperature, resulting in drops in oxygen use, CO2 production, and drug clearance. To combat the decrease in metabolic rate, physiologic shivering can drastically increase core temperature and prevent or slow induction of MTH. Sedation and paralysis must be optimized to combat shivering, which can be achieved by using neuromuscular blockers, sedatives, alpha-2 agonists, magnesium sulfate, and opioids. Table 1 includes a list of commonly used anti-shivering agents. Ventilator settings also need to be continuously reassessed to prevent relative hyperventilation from the drop in CO2 production. Additionally, arterial blood gases (ABGs) drawn on cooled patients will only be accurate if measured at core body temperature, and will be inaccurate if warmed and measured at 37°C. Table 2 outlines a useful method for estimating a hypothermic ABG value warmed to 37°C.2
When considering MTH effects on hemodynamics, the normal cardiovascular system responds to cold temperatures and decreased metabolic rate with bradycardia and increased systemic vascular resistance, which counterbalance one another. Electrocardiographic manifestations commonly encountered include a slow heart rate and prolonged PR, QRS, and QT durations. Osborn or J waves are occasionally observed. Rapid cooling causes increased diuresis through tubular dysfunction, leading to hypovolemia and urinary loss (and/or intracellular shifts) of magnesium, phosphate, calcium, and potassium. This loss of volume can decrease CO2 production and increase the risk for other dysrhythmias when coupled with the loss of electrolytes. These complications can be prevented with chilled saline volume replacement, monitoring of urinary output, serial measurements of electrolytes, and replacing electrolyte levels to achieve normal values. As previously noted, antidysrhythmics and vasopressors can be considered, if necessary; however, healthcare providers must remember that MTH may alter the pharmacokinetics of each drug. Hypothermia may also further exacerbate hyperglycemia by inducing insulin resistance, so insulin needs may be increased.
Coagulation abnormalities have been associated with MTH. Temperatures <35°C tend to cause isolated platelet dysfunction, while lower temperatures (<33°C) tend to cause factor dysfunction.2 However, investigators who studied these effects during MTH and thrombolysis found that most cases involved very mild platelet dysfunction, which did not increase the risk of bleeding any more than the standard risk associated with thrombolysis.19 Concern over bleeding risks should not prevent therapy with MTH, and use of packed red cells, platelets, or factors can be considered, if needed. Low-dose desmopressin has also been found to reverse MTH-associated platelet dysfunction.20
During the rewarming phase, the patient’s metabolic rate increases. If rewarming occurs too quickly, all benefits of MTH can be lost. In addition, constant attention is needed to prevent acid/base and electrolyte abnormalities (ie, hyperkalemia). If rewarming occurs slowly, the body can mitigate these challenges with little help.
MTH and “controlled normothermia” have been shown to increase the risk of infection through the impairment of temperature-dependent proinflammatory mediators and blockade of pyrexia.2 Mediators that herald infection, such as elevated white blood cell count and C-reactive protein (CRP) levels, are unreliable. The ED physician must be vigilant regarding infection prevention and identification. Since these patients will be intubated and have multiple catheter types (eg, venous, arterial, urinary) in the presence of MTH-induced immunosuppression, it would be reasonable to maintain a high index of suspicion for the development of certain common nosocomial infections, including hospital-acquired or ventilator-associated pneumonia and urinary tract infections. An initial set of blood cultures and prophylaxis with broad-spectrum antibiotics should be considered. When patient stability allows, serial physical examinations looking for cutaneous signs of infection and decubitus ulcers should be considered, along with frequent assessment of all catheter sites. Another sign that might indicate the presence of infection is the sudden increased workload of cooling devices, as shown by a sudden increase in body temperature or difficulty maintaining a certain body temperature.2
Coronary Reperfusion with Angiography and PCI
Acute coronary syndromes (ACSs) are well-known as the most common cause of cardiac arrest, with 60% to 80% of cases resulting from cardiovascular disease.21 Immediate angiography along with PCI has remained the only intervention that independently predicts good survival outcomes in this setting.13,15,16,22-26 Of critical importance to properly implementing this systems-of-care approach, is that ED physicians are cognizant of the indications of early PCI in standardized, post-resuscitation care. More specifically, several questions need to be examined:
1. Who should get coronary angiography and PCI?
2. When should PCI be initiated?
3. Is thrombolysis a safe alternative or is transfer to a PCI center warranted?
Who Should Get Coronary Angiography and PCI?
To best identify potential candidates for PCI, the post-ROSC 12-lead electrocardiogram (ECG) should be obtained as soon as patient care allows. In many cases, an ECG will show evidence of ST-segment elevation myocardial infarction (STEMI), indicating a clear need for coronary angiography and PCI. However, the absence of ST-segment changes on an ECG does not rule out ACS, and coronary angiography may be warranted to determine the need for coronary reperfusion with PCI. What follows is a brief review of the role of coronary angiography and PCI for the STEMI and non-STEMI patient.
STEMI. One large case series11 that studied post-ROSC OHCA patients who underwent PCI after meeting STEMI criteria based on their ECG findings revealed that 60% survived to hospital discharge, with 86% being neurologically intact. Patients included in this case series were a mix of awake, comatose, young, and elderly. Several of the reports making up this case series led the American Heart Association (AHA) and the International Liaison Committee on Resuscitation (ILCOR) in 2010 to provide recommendations that all patients with STEMI and/or new left bundle branch block after ROSC be considered for early angiography with PCI.22,26 This recommendation enabled both organizations to stand behind their position that mental status should not preclude anyone from receiving PCI, as even comatose patients can have excellent long-term neurologic outcomes following reperfusion therapy.
Non-STEMI. Because ECG data and clinical signs can be poor predictors of coronary ischemia in post-ROSC OHCA patients, and ST changes on ECG are not sensitive enough for detecting ACS in this population,27 those without ECG evidence of STEMI should also be considered for immediate coronary angiography and PCI.24 Based on the limitations of ECG data, many investigators recommend undertaking coronary angiography and PCI regardless of ECG findings.13,24,27,28 to check for coronary lesions, often suspected to be the cause of the cardiac arrest. Despite having no evidence of ACS on their ECG, studies have found a notable percentage of patients showing clear angiographic evidence of coronary occlusion or culprit lesions.27,29
Some clinicians fear that performing angiography—only to find complete absence of ACS—is a waste of time and resources. However, given the burden of ACS in the otherwise undifferentiated OHCA patient population, and the poor negative predictive value associated with ECG data, establishing normal coronary anatomy is a huge benefit, enabling the clinician to safely rule out ACS and move on to other therapeutic strategies.21 These studies, in addition to the 2010 AHA and ILCOR recommendations, suggest that early angiography and PCI should be considered in post-ROSC patients regardless of their ECG findings or clinical data.22
When should PCI be initiated?
Few data are available on how specific timing for angiography and PCI affects outcomes in the post-ROSC setting.11 To the best of our knowledge, no studies exist regarding the best time to initiate PCI. Some have discussed creating a similar “door-to-balloon time” approach, as in the care of ACS patients; however, given that patients need to be relatively stable before PCI, this concept may be a challenge, particularly considering the critically ill nature of the post-ROSC population. Because ACS is the most common etiology of OHCA, it seems reasonable to implement reperfusion strategies as soon as possible to preserve myocardial function, provided the patient is stable enough.
Is thrombolysis a safe alternative or is transfer to a PCI center warranted?
If PCI is not available, thrombolysis is recommended for confirmed STEMI patients only, as long as there are no contraindications to this therapy.22,26 In most cases, the risk of bleeding when combining MTH with thrombolysis is no greater than the risk of bleeding with thrombolysis alone.19 In those where the ECG is nondiagnostic for ACS, however, transfer to a PCI facility is recommended because the risks of thrombolysis outweigh the benefits.
Combining Mild Therapeutic Hypothermia with PCI
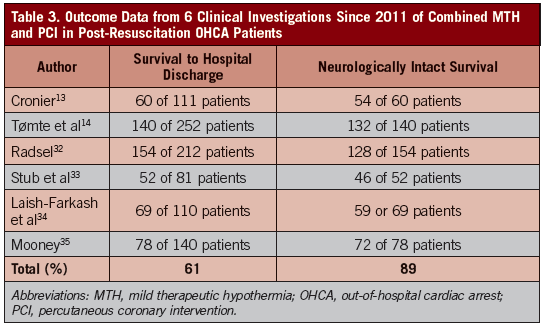
MTH and PCI should be combined to provide the most optimal post-resuscitation care available. Historically, many healthcare providers feared that MTH might delay PCI, increase the technical risk of PCI, or cause side effects that increase the risk of morbidity and mortality during or after PCI. Although MTH does carry a risk of bleeding and dysrhythmias, recent investigations have found that little risk actually exists, and that combining these 2 therapies is safe and feasible.12,18,19,25,30,31 MTH has not proven an association with excessive risks of bleeding compared with thrombolysis alone, and any bleeding risk present with PCI, is more likely associated with the anticoagulants and platelet inhibitors used.19 A study of dysrhythmias and overall cardiac and neurological risk of using MTH during PCI concluded that providing both therapies together is safe and feasible.25 Outcome data from 6 studies published since the start of 2011 showed that the MTH and PCI combination is not only safe, but also improves overall survival to hospital discharge, with a higher likelihood of neurologically intact survival (Table 3).13,14,32,33-35
Cumulatively, these studies show a survival rate of 61% to hospital discharge, with a favorable neurologic status in 89%. Though it is unclear what these patients’ neurologic function was at 1 year, but a similar study sheds light on longer-term outcomes with MTH and PCI, comparing prognoses at 1 year and 5 years post-treatment with this combination.16 When stratifying post-ROSC patients into 1 of 4 groups (ie, neither MTH or PCI; MTH alone; PCI alone; MTH and PCI), the group receiving MTH and PCI had the highest survival estimates at 1 and 5 years (P<.001).16 With these impressive statistics, few can argue that the most optimal approach to post-resuscitation care involves the combination of MTH and early PCI for all patients initially resuscitated from OHCA.
Conclusion
Many different healthcare providers deliver post-resuscitation care, from the EMS personnel in the field to the ED physicians, critical care nurses, and interventional cardiologists at the hospital. The systems-of-care approach to post-resuscitation care outlined in this 2-part article supports a multidisciplinary approach to care that emphasizes the importance of EGDT, including hemodynamic optimization, neuroprotective measures, and reperfusion therapies. When standardized care is provided to OHCA patients through a systems-of-care approach, prompt, seamless, and effective treatment is more likely to be provided. For a framework on designing a systems-of-care approach, turn to page 169 to see the tip sheet, “5 Important Elements to Consider When Designing a Systems-of-Care Approach to Treat Resuscitated Patients After Sudden Cardiac Arrest.”

John P. Benner, DO, NREMT-P, was a graduate of the Edward Via College of Osteopathic Medicine in Blacksburg, VA.
David R. Burt, MD, is associate professor of emergency medicine at the University of Virginia and medical director of the Chest Pain Observation Unit at the University Medical Center, both in Charlottesville, VA.
James E. Powers, DO, is associate dean for clinical academic affairs, associate professor of emergency medicine, and chair of emergency medicine at the Edward Via College of Osteopathic Medicine in Blacksburg, VA.
William J. Brady, MD, is a professor of emergency medicine at the University of Virginia, as well as chair of the University Medical Center Resuscitation Committee and operational medical director with Albemarle County Fire Rescue, both in Charlottesville, VA.
References:
1. The Hypothermia After Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346(8):549-556.
2. Polderman KH. Mechanisms of action, physiological effects, and complications of hypothermia. Crit Care Med. 2009;37(suppl 7):S186-S202.
3. Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346(8):557-563.
4. Hörburger D, Testori C, Sterz F, et al. Mild therapeutic hypothermia improves outcomes compared with normothermia in cardiac arrest patients–a retrospective review. Crit Care Med. 2012;40(8):2315-2319.
5. Larrson IM, Wallin E, Rubertsson S. Cold saline infusion and ice packs alone are effective in inducing and maintaining therapeutic hypothermia after cardiac arrest. Resuscitation. 2010;81(1):15-19.
6. Larabee TM, Campbell JA, Severyn FA, et al. Intraosseous infusion of ice cold saline is less efficacious than intravenous infusion for induction of mild therapeutic hypothermia in a swine model of cardiac arrest. Resuscitation. 2011;82(5):603-606.
7. Gillies MA, Pratt R, Whiteley C, et al. Therapeutic hypothermia after cardiac arrest: a retrospective comparison of surface and endovascular cooling techniques. Resuscitation. 2010;81(9):1117–1122.
8. Peberdy MA, Callaway CW, Neumar RW, et al. Part 9: post-cardiac arrest care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(suppl 3):S768-S786.
9. Weingart SD, Mayer SA, Polderman KH. Rectal probe temperature lag during rapid saline induction of hypothermia after resuscitation from cardiac arrest. Resuscitation. 2009;80(7):837-838.
10. Nolan JP, Neumar RW, Adrie C, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A scientific statement from the international liaison committee on resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation. 2008;79(3):350-379.
11. Kern KB. Viewpoint: optimal treatment of patients surviving out-of-hospital cardiac arrest. JACC Cardiovasc Interv. 2012;5(4):597-605.
12. Knafelj R, Radsel P, Ploj T, et al. Primary percutaneous coronary intervention and mild induced hypothermia in comatose survivors of ventricular fibrillation with ST-elevation acute myocardial infarction. Resuscitation. 2007;74(2):227-234.
13. Cronier P, Vignon P, Bouferrache K, et al. Impact of routine percutaneous coronary intervention After out-of-hospital cardiac arrest due to ventricular fibrillation. Critical Care. 2011;15:R122.
14. Tømte Ø, Andersen GØ, Jacobsen D, et al. Strong and weak aspects of an established post-resuscitation protocol–a five-year observational study. Resuscitation. 2011;82(9):1186-1193.
15. Sunde K, Pytte M, Jacobsen D, et al. Implementation of a standardised treatment protocol for post-resuscitation care after out-of-hospital cardiac arrest. Resuscitation. 2007;73(1):29-39.
16. Dumas F, White L, Stubbs BA, et al. Long-term prognosis following resuscitation from out-of-hospital cardiac arrest: role of percutaneous coronary intervention and therapeutic hypothermia. JACC. 2012;60(1);21-27.
17. Naples R, Ellison E, Brady WJ. Cranial computed tomography in the resuscitated patient with cardiac arrest. Am J Emerg Med. 2009;27(1):63-67.
18. Gräsner JT, Meybohm P, Caliebe A, et al. Postresuscitation care with mild therapeutic hypothermia and coronary intervention after out-of-hospital cardiopulmonary resuscitation: a prospective registry analysis. Critical Care. 2011;15:R61.
19. Schefold JC, Storm C, Joerrs A, et al. Mild therapeutic hypothermia after cardiac arrest and the risk of bleeding in patients with acute myocardial infarction. Int J Cardiol. 2009;132(3):387-391.
20. Ng KF, Cheung CW, Lee Y, et al. Low-dose desmopressin improves hypothermia-induced impairment of primary haemostasis in healthy volunteers. Anaesthesia. 2011;66(11):999-1005.
21. Reynolds JC, Callaway CW, El Khoudary SR, et al. Coronary angiography predicts improved outcome following cardiac arrest: propensity-adjusted analysis. J Intensive Care Med. 2009;24(3):179-186.
22. O’Connor RE, Bossaert L, Arntz H-R, et al. Part 9: acute coronary syndromes: 2010 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2010;122(Suppl 2):S422-465.
23. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368-1377.
24. Spaulding CM, Joly LM, Rosenberg A, et al. Immediate coronary angiography in survivors of out-of-hospital cardiac arrest. N Engl J Med. 1997;336:1629-1633.
25. Batista LM, Lima FO, Januzzi jr JL, et al. Feasibility and safety of combined percutaneous coronary intervention and therapeutic hypothermia following cardiac arrest. Resuscitation. 2010;81:398-403.
26. O’Connor RE, Brady WJ, Brooks SC, et al. Part 10: acute coronary syndromes: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(suppl 3):S787-S817.
27. Anyfantakis FA, Baron G, Aubry P, et al. Acute coronary angiographic findings in survivors of out-of-hospital cardiac arrest. Am Heart J. 2009;157:312-318.
28. Kern KB, Rahman O. Emergency percutaneous coronary intervention for resuscitated victims of out-of-hospital cardiac arrest. Catheter and Cardiovasc Interv. 2010;75:616-624.
29. Dumas F, Cariou A, Manzo-Silberman S, et al. Immediate percutaneous coronary intervention is associated with better survival after out-of-hospital cardiac arrest: insights from the PROCAT (Parisian Region Out-of-Hospital Cardiac ArresT) Registry. Circ Cardiovasc Interv. 2010;3(3):200-207.
30. Wolfram S, Pierau C, Radke PW, et al. Mild therapeutic hypothermia in patients after out-of-hospital cardiac arrest due to acute ST-segment elevation myocardial infarction undergoing immediate percutaneous coronary intervention. Crit Care Med. 2008;36(6):1780-1786.
31. Hovdenes J, Laake JH, Aaberge L, et al. Therapeutic hypothermia after out-of-hospital cardiac arrest: experiences with patients treated with percutaneous coronary intervention and cardiogenic shock. Acta Anaesthesiol Scand. 2007;51:137-142.
32. Radsel P, Knafelj R, Kocjancic S, et al. Angiographic characteristics of coronary disease and post-resuscitation electrocardiograms in patients with aborted cardiac arrest outside a hospital. Am J Cardiol. 2011;108(5):634-638.
33. Stub D, Hengel C, Chan W, et al. Usefulness of cooling and coronary catheterization to improve survival in out-of-hospital cardiac arrest. Am J Cardiol. 2011;107:522–527.
34. Laish-Farkash A, Matetzky S, Oieru D, et al. Usefulness of mild therapeutic hypothermia for hospitalized comatose patients having out-of-hospital cardiac arrest. Am J Cardiol. 2011;108(2):173-178.
35. Mooney MR, Unger BT, Boland LL, et al. Therapeutic hypothermia after out-of-hospital cardiac arrest: evaluation of a regional system to increase access to cooling. Circulation. 2011;124(2):206-214.