
Not Your Usual Suprasellar Mass
History
 A 71-year-old female with a past medical history of hypertension presented to the emergency department with an 8-week history of neurological symptoms including confusion, short-term memory loss, and progressive weakness. Labwork revealed severe hypercalcemia (15.3 mg/dL [range: 8.5-10.5 mg/dL]), moderate anemia (hemoglobin levels at 9.5 g/dL [range: 11.5-15.5 g/dL]), and mild kidney insufficiency (creatinine levels at 1.47 mg/dL [range: 0.70-1.40 mg/dL]). An outpatient CT of the head revealed a mass within the sella turcica (Figure 1). She was consequently hospitalized for evaluation.
A 71-year-old female with a past medical history of hypertension presented to the emergency department with an 8-week history of neurological symptoms including confusion, short-term memory loss, and progressive weakness. Labwork revealed severe hypercalcemia (15.3 mg/dL [range: 8.5-10.5 mg/dL]), moderate anemia (hemoglobin levels at 9.5 g/dL [range: 11.5-15.5 g/dL]), and mild kidney insufficiency (creatinine levels at 1.47 mg/dL [range: 0.70-1.40 mg/dL]). An outpatient CT of the head revealed a mass within the sella turcica (Figure 1). She was consequently hospitalized for evaluation.
Assessment
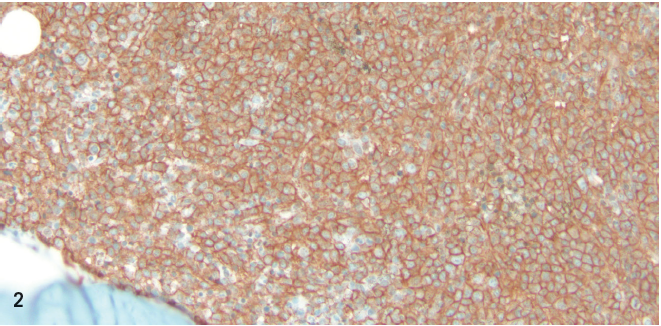
A skeletal survey revealed innumerable small lytic lesions throughout the skeleton, most prominent within the skull. A bone marrow biopsy was performed and demonstrated findings consistent with kappa chain multiple myeloma. Given the presence of a suprasellar mass, pituitary function was assessed and no significant abnormalities were found. Transsphenoidal biopsy of the sphenoid mass was performed; the pathology report revealed neoplastic cells strongly positive with antibodies to CD138 and kappa light chains, consistent with plasma cell neoplasm (Figure 2). She was consequently diagnosed with multiple myeloma.
Discussion
Multiple myeloma is a well-recognized neoplastic plasma cell disorder. Diagnostic criteria for multiple myeloma have been published and disseminated, and is based on bone marrow biopsy revealing typically at least 10% clonal bone marrow plasma cells as well as presence of monoclonal protein in the serum or urine. Organ dysfunction related to myeloma includes anemia, renal impairment, and bony disease.1
Clinical findings noted during presentation include: anemia at 73% to 85.3%,2,3 fatigue at 32%,3 weight loss at 24%,3 renal impairment (Cr ≥2g/dL): ~20%,3,4 bone lytic lesions at 67%,3 bone pain at 58%3, and hypercalcemia (≥ 11mg/dL): 13%.3
Severe hypercalcemia may produce changes in cognitive function. Intracranial involvement of multiple myeloma is rare and typically arises from osseous involvement of the cranial vault, skull base, nose, or paranasal sinuses.5,6 Often, such masses are misdiagnosed as nonfunctioning pituitary adenomas. Biopsy facilitates diagnostic confirmation.
Present in 1% of cases, leptomeningeal involvement of multiple myeloma is particularly rare and devastating. Dissemination of plasma cells into the CNS is thought to occur through hematogenous spread or as an extension of involved adjacent bony tissue.7
A case series of multiple myeloma patients with CNS complications revealed a strong association with translocations and deletions in chromosome 13.8 Poorer prognosis associated with a high B-microglobulin level and several chromosomal abnormalities,9 including specific translocations including t(4;14), deletion 17p13, and chromosome 1 abnormalities.10 It is possible that myeloma patients with intracranial involvement represent a subset of these high risk individuals with poor prognosis. No systematic review of cytogenetic abnormalities in multiple myeloma associated with CNS involvement has been conducted to date.
Outcome of the Case
The patient underwent treatment of her multiple myeloma with melphalan, bortezumab, and prednisone. Follow-up CT of the head demonstrated absence of the suprasellar mass following chemotherapy.
1.International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: A report of the international myeloma working group. Br J Haematol. 2003;121(5):749-757.
2.Birgegard G, Gascon P, Ludwig H. Evaluation of anaemia in patients with multiple myeloma and lymphoma: Findings of the European Cancer Anemia Survey. Eur J Haematol. 2006;77(5):378-386.
3.Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33
4.Eleutherakis-Papaiakovou V, Bamias A, Gika D, et al. Renal failure in multiple myeloma: Incidence, correlations, and prognostic significance. Leuk Lymphoma. 2007;48(2):337-341.
5.Cerase A, Tarantino A, Gozzetti A, et al. Intracranial involvement in plasmacytomas and multiple myeloma: a pictorial essay. Neuroradiology. 2008;50(8):665-674.
6.Yaman E, Benekli M, Coskun U, et al. Intrasellar plasmacytoma: an unusual presentation of multiple myeloma. Acta Neurochir (Wien). 2008;150(9):921-924.
7.Leifer D, Grabowski T, Simonian N, Demirjian ZN. Leptomeningeal myelomatosis presenting with mental status changes and other neurologic findings. Cancer. 1992;70(7):1899-1904.
8.Fassas AB, Ward S, Muwalla F, et al. Myeloma of the central nervous system: Strong association with unfavorable chromosomal abnormalities and other high-risk disease features. Leuk Lymphoma. 2004;45(2):291-300.
9.Greipp PR, San Miguel J, Durie BG, et al. International staging system for multiple myeloma. J Clin Oncol. 2005;23(15):3412-3420.
10.Avet-Loiseau H, Attal M, Moreau P, et al. Genetic abnormalities and survival in multiple myeloma: The experience of the intergroupe francophone du myelome. Blood. 2007;109(8):3489-3495.