
Individuals With Autism Spectrum Disorder: A Study of the Age of Attaining Daytime Dryness
Authors:
Victoria J. Faulkner, PhD; G. Thomas Schanding Jr, PhD; Weihua Fan, PhD; and Gerald E. Harris, PhD
Citation:
Faulkner VJ, Schanding T, Fan W, Harris GE. Individuals with autism spectrum disorder: a study of the age of attaining daytime dryness. Consultant. 2017;57(7):394-398.
ABSTRACT: Successful completion of toilet training is an essential adaptive skill and a key milestone. Data from 583 children with an autism spectrum disorder (ASD) diagnosis confirmed by the Simons Simplex Collection were examined regarding their age at attainment of daytime dryness using the Autism Diagnostic Interview–Revised and compared with a model for attaining daytime dryness. Results from χ2 analysis indicated that children with ASD were much more likely to be delayed in achieving the developmental milestone of daytime dryness.
KEYWORDS: Autism spectrum disorder, toilet training, bladder control
Autism spectrum disorder (ASD) affects approximately 1 in 68 children in the United States.1 According to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, ASD is associated with impairment in social communication and social interaction as well as restricted, repetitive patterns of behavior, interest, or activities.2 Many children with ASD struggle to acquire adaptive behavior skills, including socialization, communication, and daily living skills.3
A deficit in adaptive behaviors, especially daily living skills, including toileting skills, may contribute to an individual’s prognosis and to his or her level of independent functioning. Children with ASD may have difficulty with the toilet training process, which affects whether and when they will achieve daytime dryness.4 When toilet training success is delayed or never achieved, it can cause long-term stress for families.5 Despite the noted difficulty and stress associated with toilet training, there continues to be a very limited amount of research about it in association with ASD.6
The study described here investigated the average age of achieving daytime dryness within the ASD population compared with the general population.
Toilet Training and ASD
Children with ASD may have difficulties obtaining toilet training skills, but there is a lack of information as to why these difficulties may exist. The level of cognitive and verbal abilities may be a factor that affects the likelihood of success.4 Individuals with ASD often have difficulties with transitions and generalizing activities to different settings.7 Children with ASD may also have different sensory experiences than persons without ASD.7,8 For example, some children with ASD may experience acute sensitivity from articles of clothing, which would make changing in and out of clothing during the toilet training process uncomfortable and aversive; others may become distracted or overwhelmed by environmental stimulation in different bathrooms.9 In addition, communication is an important element in the training process. Without the adequate receptive language needed to understand and learn instructions and the expressive communication needed to convey needs, toilet training can be very difficult.
Average Age of Toilet Training Success
Not all children obtain continence at the same time; therefore, there is not a set age at which to begin toilet training. Early studies suggested that a child at the age of 20 months may be able to be toilet trained.10 Bloom and colleagues11 determined that children were successfully toilet trained between the ages of 9 months and 5 years, with an average age of 2.4 years (standard deviation [SD], 7.2 months), although more recent data indicate that toilet training is occurring later than that.12
In regard to normal toileting milestones, children will begin to show signs of readiness at 18 months, training is recommended to begin at 24 months, and most children will have achieved successful daytime continence by 30 to 36 months.13 Data reported in 1968 from a 12-year longitudinal study by Oppel and colleagues14 revealed that in a sample of 859 children, when controlling for race, sex, and prematurity, 95% of children achieved daytime dryness by 5 years (SD, 10.8 months), with 99% having achieved daytime dryness by 10 years (SD, 4.8 months), and 100% achieved daytime dryness by 12 years (SD, 3.6 months). In examining children with ASD, Tsai and colleagues15 in 1981 noted that 59% of boys with ASD and 86% of girls with ASD exhibited daytime enuresis after the age of 3½ years. Lowenthal16 noted that children with developmental delays may not achieve bladder control until 4 years of age; however, Azrin and Foxx10 suggested delaying the start of toilet training for children with intellectual disabilities until they are at least 30 months old or up to 5 years old if they are severely delayed, with an IQ of approximately 30. It is not known whether children who have a diagnosis of ASD fit this same timeframe model.
Importance of Toilet Training Success
There are great incentives for successfully achieving toileting skills: increased overall hygiene, admittance to childcare facilities and activities, and, in general, a greater quality of life.5 Children who are properly toilet trained obtain a new sense of independence,7 which may generalize to other self-help skills such as feeding and dressing.10 There are also medical benefits to consider. Using a toilet, rather than changing diapers, can reduce the opportunity of coming into contact with viruses such as rotavirus and parasites such as Giardia lamblia, both of which can cause severe diarrhea.17
Before the toilet training process can begin, parents and caregivers have to assess the child’s readiness. Regardless of age, a child must demonstrate bladder control, physical development, and instructional readiness.10,18 To be considered successfully toilet trained, a child must demonstrate a series of steps. He or she must have the cognitive ability to understand the expectation, to recognize the feeling of a full bladder, and to physically empty his or her bladder in a toilet.19 A child with bladder control will be able to release urine in a single urination rather than leaking small amounts of urine and will remain dry for several hours. The child must also demonstrate adequate fine and gross motor skills. Additional indicators of toilet training readiness include the following: imitates parents’ behavior, is able to pull clothes up and down, indicates first when he or she is “going” (urinating or defecating), and when he or she needs to “go.”20 Deficits associated with ASDs in the areas of imitation of others, expressive/receptive communication, and motor skills may hinder the toilet training process for children with ASD.
It is also unknown whether parents and clinicians can expect children with ASD to achieve daytime dryness within the same timeframe as the general population. Given the lack of research examining children with ASD and daytime dryness, we attempted to answer the following question: When compared with Oppel and colleagues’ model,14 do children with an ASD diagnosis fit the typical age range for developing daytime dryness? It was hypothesized that children with ASD will not achieve daytime dryness within the same time periods as typically developing children.
NEXT: Method, Measures, Results, Discussion
Method: Participants
This study was approved by the Committee for the Protection of Human Subjects at the first author’s university, and a request for data was approved by the Simons Foundation Autism Research Initiative Base. The participant sample comprised more than 2000 children of families who participated in the Simons Simplex Collection (SSC; https://sfari.org/resources/autism-cohorts/simons-simplex-collection). To qualify for inclusion in the SSC, families must meet strict research criteria.21 Specifically, families must have 1 child who has received a diagnosis of an ASD and who is at least 4 years of age, with 1 or more siblings without an ASD diagnosis and who are at least 4 years of age, and both biological parents who do not have an ASD diagnosis. Participants were excluded if the child did not meet the diagnostic criteria for ASD, if the child’s relatives were determined to have ASD, if there were perinatal complications, or if the child had a nonverbal mental age that was 18 months or below. Informed consent for participation in the SSC was obtained from the parents, and assent was obtained from the children.
For the current wave of data analyzed, 2744 children were included in the database; however, certain participants were excluded. Only those children who were 144 months (12 years) or older at the time of data collection were included to examine the age of attainment of dryness. Those participants who had the code of 996 or 997 on the Autism Diagnostic Interview–Revised (ADI-R)22 Acquisition of Daytime Bladder Control item were excluded from the study, because this code indicated that it was not known whether the participant had achieved bladder control. The majority of the 2156 children excluded from the study were below the age of 144 months. Two participants were excluded because of missing toilet training information. One participant was excluded because the age of achieving daytime dryness was 3 months and was judged to be an extreme outlier or a possible data-entry error. A total of 583 children met criteria for the study.
As indicated, all participants met the criteria for an ASD. The majority were boys (84.8%) and white (74.8%). Approximately 84% of the participants identified as non-Hispanic. Of those families providing data about annual income, approximately 15% of participants’ families reported annual household incomes of $50,000 or less, 40% reported incomes from $51,000 to $100,000, and 40% reported annual earnings greater than $101,000 (Table 1). In considering the level of educational attainment of mothers and fathers, the majority completed a baccalaureate or graduate degree (56.9% of fathers, 55.8% of mothers).

Measures
Families who participated in the SSC completed several phenotypic measures to obtain comprehensive and diagnostic data. For the purpose of this study, information from the ADI-R was analyzed. The ADI-R provides a diagnostic algorithm for autism based on an interview of parents or caregivers. The ADI-R includes early development questions that focus on milestones such as walking, talking, and toilet training. The researcher codes the child’s age in months at the time of the last daytime accident before a 12-month period of no accidents (operational definition of achieving daytime dryness). The researcher can also code for whether the child had been toilet trained and has now regressed, if he or she had never been considered toilet trained, or if he or she is currently toilet training but has not yet reached 12 months with no accidents (item No. 6 from the ADI-R, Acquisition of Bladder Control–Daytime). Utilizing the ADI-R question of parent self-report of their child’s attainment of daytime dryness mirrored the methodology of Oppel and colleagues in ascertaining daytime dryness. Only those participants who were fully trained with no regression were included in the analysis.
Results
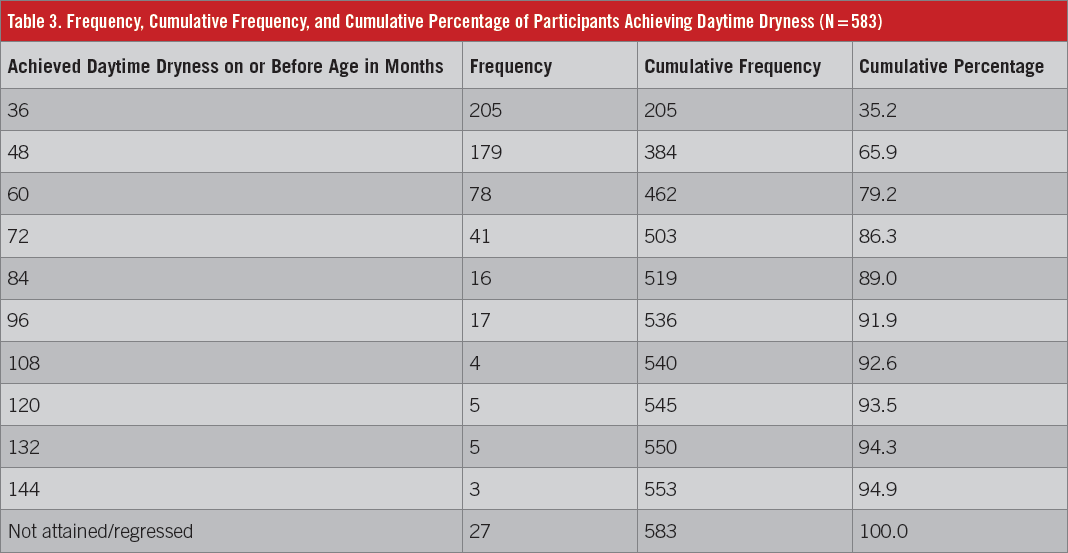
A χ2 goodness-of-fit test was used to determine whether children with ASD achieved daytime dryness in the same timeframe as typically developing children based on the findings of Oppel and colleagues. Based on the percentage of participants who attained daytime dryness in the Oppel study, expected percentages were calculated from the current sample of children with ASD (ie, expectation of 95% of the current sample children at age 5 = 553 – 583 × 95%). The observed and expected data are shown by age group in Table 2. Table 3 provides the frequencies of children who achieved dryness by age (in months). A total of 27 participants were determined not to have achieved daytime dryness. Of those 27 children, 6 had initially achieved dryness then regressed and had urinary accidents regularly, 15 were reported to have never achieved daytime continence, and 6 had been continent for a period of less than 12 months currently.
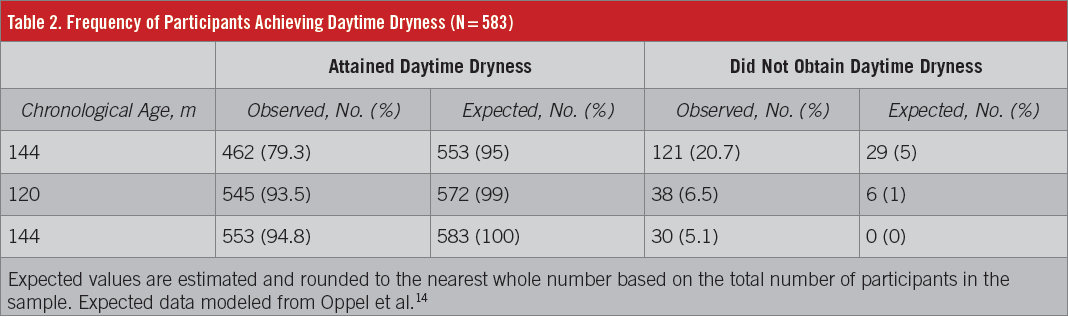
In examining the attainment of daytime dryness, children with ASD were less likely than the general population to attain this developmental milestone at 60 months (5 years). A χ2 goodness-of-fit test indicated that approximately 79% of children with an ASD attained dryness by 60 months whereas 95% of same-age neurotypical peers attain dryness at this age, χ2 (1, N = 583) = 307.14, P < .001 (κ = .72). In examining attainment of this milestone at 10 years of age, approximately 93% of children with ASD attained daytime dryness, a lower portion of children compared with same-age neurotypical peers, χ2 (1, N = 583) = 172.44, P < .001 (κ = .56). At age 12, 5.1% of children with ASD had not attained daytime dryness; however, an additional 3 participants attained daytime dryness after age 12 in this sample (not accounted for in Table 3).
Discussion
This study examined the age at which children with diagnosed ASD attained daytime dryness compared with typically developing children. Overall, children with ASD were significantly delayed in attaining this developmental milestone when compared with the Oppel et al model. Accordingly, 95% of the sample would be expected to achieve daytime dryness by age 5, 99% by age 10, and 100% by age 12; however, the current data indicate that only 79.3% of the sample had achieved daytime dryness by age 5, 93.5% by age 10, and 94.9% by age 12. By contrast, a larger percentage (14% compared with 4% in the general population) of children with ASD achieve daytime dryness between the age of 5 and 10. Additionally, approximately 5% of children with ASD were not dry by the age of 12. When considering the results of Blum et al,12 typically developing children achieve daytime dryness at approximately 36 months; however, only 35% of children with ASD attained dryness by 36 months.
A strength of this study is the use of a standardized measure, the ADI-R, to collect data regarding developmental milestones. It should be noted that the criteria for success in achieving daytime dryness are stricter using the ADI-R (ie, 12 months of daytime continence with no accidents) compared with previous studies. Blum et al12 defined success in daytime toilet training as completed when parents reported the child wears underwear during the day and urinates/defecates in the toilet or potty with fewer than 4 urine accidents per week and 2 or fewer episodes of fecal soiling per month. Oppel et al14 defined daytime dryness success as a parent reporting an initial period of dryness, wetting less often than once a month, for either daytime or nighttime. The more stringent criteria for dryness from the ADI-R may account for some of the differences between the results obtained by Oppel et al. The more demanding criteria of no accidents for 12 months may better demarcate successful attainment of daytime dryness; however, this may not fully account for accidents such as a child having difficulty with removing clothing, illness, being too distant from a toilet, or other acute stressors as noted by Brazelton and colleagues.23
Our study examined only the attainment of daytime dryness for individuals with ASD and did not examine factors associated with attaining that milestone. Further research should be conducted to investigate the factors associated with a success or delay in toilet training for children with ASD, such as compounding issues of intellectual impairment, restricted/repetitive behaviors, communication difficulties, motor difficulties, and severity/impairment of ASD condition.
While the SSC contains a highly reliable set of data for children with ASD, the generalizability of this data should be viewed with some caution. First, the sample contained a disproportionately high number of white, non-Hispanic boys. Secondly, the sample contains families with a fairly high educational background and income level. The families included in this study may have better access to intervention services than those families with less education and less income. Also, families with lower incomes may have additional pressure to toilet train a child faster (eg, the need to train children to reduce expenses such as diapers). Future research could use a sample that is more reflective of the general US population.
The results of this study create a better understanding of the timeframe for achieving daytime dryness for children with a diagnosis of ASD. Parents and clinicians should be aware that children with ASD may not achieve daytime dryness within the same timeframe as typically developing children. A smaller percentage of children in the ASD population may achieve daytime dryness by the age of 5. However, when compared with typically developing children, a greater percentage of children in the ASD population will achieve daytime dryness between the ages of 5 and 10.
It is important to note that there was not a 100% success rate within the ASD sample. Some children with ASD are not toilet trained by the age of 12, possibly impacting their school placement, their ability to be included in social activities, and their level of independent functioning. Understanding that children in the ASD population may achieve toilet training skills in a different timeframe may help parents and clinicians have more reasonable expectations and set more appropriate goals.
Victoria J. Faulkner, PhD, is a licensed specialist in school psychology in the Special Services Department at Deer Park Independent School District in Deer Park, Texas.
G. Thomas Schanding Jr, PhD, is an associate professor in the Department of Clinical Health and Applied Sciences at the University of Houston–Clear Lake in Houston, Texas.
Weihua Fan, PhD, is an associate professor in the Department of Psychological, Health, and Learning Sciences at the University of Houston in Houston, Texas.
Gerald E. Harris, PhD, is the executive director of the Center for Forensic Psychology and the training director of Forensic Psychology Services in the Department of Psychology at the University of Houston in Houston, Texas.
Acknowledgments: The authors are grateful to all of the families at the participating SSC sites, as well as the principal investigators (A. Beaudet, R. Bernier, J. Constantino, E. Cook, E. Fombonne, D. Geschwind, R. Goin-Kochel, E. Hanson, D. Grice, A Klin, D. Ledbetter, C. Lord, C. Martin, D. Martin, R. Maxim, J. Miles, O. Ousley, K. Pelphrey, B. Peterson, J. Piggot, C. Saulnier, M. State, W. Stone, J. Sutcliffe, C. Walsh, Z. Warren, and E. Wijsman).
The authors also appreciate obtaining access to phenotypic data on the Simons Foundation Autism Research Initiative Base.
Approved researchers can obtain the SSC population dataset described in this study by applying at https://sfari.org.
REFERENCES:
- Christensen DL, Baio J, Braun KVN, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2012. MMWR Surveill Summ. 2016;65(3):1-23.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
- Kanne SM, Gerber AJ, Quirmbach LM, Sparrow SS, Cicchetti DV, Saulnier CA. The role of adaptive behavior in autism spectrum disorders: implications for functional outcome. J Autism Dev Disord. 2011;41(8):1007-1018.
- Dalrymple NJ, Ruble LA. Toilet training and behaviors of people with autism: parent views. J Autism Dev Disord. 1992;22(2):265-275.
- Kroeger K, Sorensen R. A parent training model for toilet training children with autism. J Intellect Disabil Res. 2010;54(6):556-567.
- Keen D, Brannigan KL, Cuskelly M. Toilet training for children with autism: the effects of video modeling category. J Dev Phys Disabil. 2007;19(4):291-303.
- Schonwald A. Toilet training: strategies for success in children with developmental disabilities. Consultant Pediatrician. 2009;8(7):254-258.
- Lane, AE, Young RL, Baker AEZ, Angley MT. Sensory processing subtypes in autism: association with adaptive behavior. J Autism Dev Disord. 2010;40(1):112-122.
- Wheeler M. Toilet Training for Individuals With Autism or Other Developmental Issues. 2nd ed. Arlington, TX: Future Horizons Inc; 2007.
- Azrin NH, Foxx RM. Toilet Training in Less Than a Day. New York, NY: Simon & Schuster; 1974.
- Bloom, DA, Seeley WW, Ritchey ML, McGuire EJ. Toilet habits and continence in children: an opportunity sampling in search of normal parameters. J Urol. 1993;149(5):1087-1090.
- Blum NJ, Taubman B, Nemeth N. Why is toilet training occurring at older ages? A study of factors associated with later training. J Pediatr. 2004;145(1):107-111.
- Stadtler AC, Gorski PA, Brazelton TB. Toilet training methods, clinical interventions, and recommendations. Pediatrics. 1999;103(6 pt 2):1359-1361.
- Oppel WC, Harper PA, Rider RV. The age of attaining bladder control. Pediatrics. 1968;42(4):614-626.
- Tsai L, Stewart MA, August G. Implication of sex differences in the familial transmission of infantile autism. J Autism Dev Disord. 1981;11(2):165-173.
- Lowenthal B. Teaching basic adaptive skills to young children with disabilities. Early Child Dev Care. 1996;115(1):77-84.
- Schmitt BD. Toilet training: getting it right the first time. Contemp Pediatr. 2004;21(3):105-122.
- Snell ME. Basic self-care instruction for students without motor impairments. In: Snell ME, ed. Systematic Instruction of Persons With Severe Handicaps. 3rd ed. Columbus, OH: Charles E. Merrill Publishing Co; 1987:334-389.
- Harris A. Toilet training children with learning difficulties: what the literature tells us. Br J Nurs. 2004;13(13):773-777.
- Toilet training guidelines: parents—the role of the parents in toilet training. Pediatrics. 1999;103(6 pt 2):1362-1363.
- Fischbach GD, Lord C. The Simons Simplex Collection: a resource for identification of autism genetic risk factors. Neuron. 2010;68(2):192-195.
- Rutter M, Le Couteur A, Lord C. Autism Diagnostic Interview–Revised. Los Angeles, CA: Western Psychological Services; 2008.
- Brazelton TB, Christophersen ER, Frauman, AC, et al. Instruction, timeliness, and medical influences affecting toilet training. Pediatrics. 1999;103(6 pt 2):1353-1358.