
How Would You Diagnose This Woman’s Repeated Chest Pains?
A 47-year-old Caucasian female was seen for the first time in a primary care clinic for multiple emergency room visits for atypical chest pain. She was having these intermittent chest pains for several months prior to her visit. She has a history of eosinophilic esophagitis and has been on a proton pump inhibitor for years. She has never had pain relating to her eosinophilic esophagitis.
Physical Examination
The patient described the chest pain as a sharp, non-radiating pain around her xiphoid process. It was sometimes associated with meals, but not consistently. She could not pinpoint the type of food that would cause the pain, and she had no associated nausea, vomiting, diarrhea, diaphoresis, or numbness. The pain was not exacerbated by exertion and only resolved with time.

Laboratory Tests
During the first occurrence of this pain, it was rated a 12 out of 10 pain and she took herself to a local ER. She had a normal EKG, chest x-ray, abdominal ultrasound, cardiac enzymes, and stress test. She was eventually discharged home with follow-up, but returned to the ER several times before her appointment without any clear cause of her atypical chest pain.
(Answer and podcast on next page)
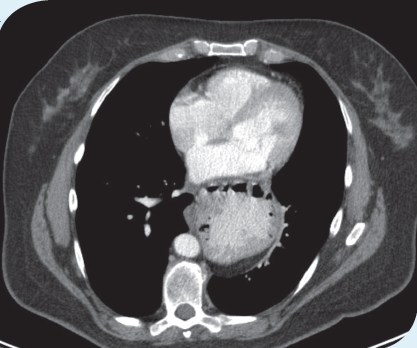
Answer: Giant hiatal hernia as a cause of intermittent chest pain
History
A 47-year-old Caucasian female was seen for the first time in primary care clinic for multiple ER visits for atypical chest pain. She was having these intermittent chest pains for several months prior to her visit. She had a normal EKG, chest x-ray, abdominal ultrasound, cardiac enzymes, and stress test. She was eventually discharged home with follow up but returned to the ER several times before her appointment without any clear cause of her atypical chest pain.
Outcome of the Case
It was believed that her chest pain was caused by either intermittent volvulus of her stomach or from mechanical compression of her stomach on her mediastinum. Hiatal hernias are often asymptomatic with type I (sliding hiatal hernias) being mostly associated with acid reflux.
Even though non-type 1 (paraesophageal hernias) are less common (5% to 15% of all hernias), they are more often associated with volvulus and a completely intrathoracicstomach.1 While in this patient there were no complications due to her hernia, non-type 1 hernias can sometimes cause serious complications such as acute gastric obstruction, incarceration, and perforation.2, 3
After her diagnosis, she was referred to general surgery and underwent a pull down of her stomach and nissen fundoplication. It was noted during the operation that her entire stomach was within her chest wall and there was even compression herleft lung. Since her surgery she has been pain-free and tolerating all types of food.
References:
1. Kahrilas PJ, Kim HC, Pandolfino JE. Approaches to the diagnosis and grading of hiatal hernia. Best Pract Res Clin Gastroenterol. 2008;22(4):601-616.
2. Dunn D, Quick G. Incarcerated paraesophageal hernia. Am J Emerg Med. 1990; 8:36-39.
3. Sihvo E, Salo J, Rasanen J, et al. Fatal complications of adult paraesophageal hernia: a population-based study. J Thorac Cardiovasc Surg. 2009;137:419-424.