
Honing Your Aesthetic Practice
ABSTRACT: As nonsurgical cosmetic procedures and anti-aging medicine continue to increase in popularity, so does the demand for qualified, ethical clinicians to provide these services, particularly among baby boomers. This article provides a brief overview of how to successfully offer medical aesthetic procedures and ensure a positive outcome for patients.
The practice of nonsurgical cosmetic aesthetics is growing at an incredible pace. In 2013, botulinum toxin aesthetic procedures rose by 15.6% from 2012. Dermal fillers such as hyaluronic acid (HA) rose by 31.5%1 The key to a successful practice is knowing your patients, knowing what to look for, providing impeccable treatments, and being aware of adverse events and how to handle them
THE CONSULT
The consult can mean the difference between success and failure for both you and your patient. The reasons someone may come to see you are limited only by the imagination. You are there to listen, observe their motions, their habits, discover what their issues are, and then guide them in the appropriate direction. Do not worry if your direction is met with disagreement by the patient. The decision to not treat a client is preferable to dealing with a client who got what they asked for, while the practitioner knew it was not the best course of action in which to proceed. That is not to say you should not listen to the patient. Of course you would not address their lips, if it is their frown that has brought them to your office. However, many patients do not understand what can be achieved with the appropriate treatment. This is why they have come to you. A good consult should result in:
•Identifying body dysmorphic disorder (BDD) traits in patients
•Acknowledgement of the variety of reasons patients want treatment
•The patient’s understanding of the fair cost of treatment because you are the expert who can treat them
•A sense of a strong relationship with you that will result in patient referrals
Body Dysmorphic Disorder
There is nothing new about BDD. This disorder has been written about and discussed for more than a century. Perhaps, it appears more prevalent today because of the huge arsenal of modalities to address both real and possibly imagined patient issues. Being aware of the warning signs of this behavior pattern is essential to avoiding practice complications associated with a patient with BDD.
Risk factors for BDD can include low self-esteem, negative childhood experiences such as teasing, a relative with the disorder, depression or anxiety, and a societal pressure to be beautiful. Some recognizable symptoms include frequent cosmetic procedures with little or no satisfaction, excessive grooming such as hair plucking or skin picking, a reluctance to be in pictures, and comparison of appearance to others or celebrities.2
Cosmetic patients will expect more of your time than a medical-based patient who is seeing you while paying perhaps a $20 copay. They do not want to be delegated to an assistant and they (hopefully) want to be a part of the decision process. These first impressions should signal that you run a patient-centered practice.3 Kent Remington, MD, agrees: “The big key is to give time to your aesthetic patients. You need to connect and engage with your patient, which will instill trust. Once you connect with them and understand what their genetics are, where they came from, what their job is and what they do—and what their real reasons are for desiring rejuvenation treatment—you can better address their concerns and achieve excellent aesthetic outcomes.”4
Naturally you will want a complete medical history along with a list of current medications, supplements, and previous use of isotretinoin.5 A direct question of possible pregnancy, lactation, and history of herpes, shingles, or cold sores is also warranted. While that list may seem obvious, many patients do not connect cold sores or shingles to herpes. Also, a list of previous cosmetic treatments and their outcome should be elicited.
Early on in the consult there may be evidence of unrealistic or even bizarre goals. If someone is already “over-the-top” with huge lips, bulging cheeks, and fan-like eyelashes, you may want to have a brief conversation about norms, and what is actually esthetically pleasing. Additionally, if someone verbalizes the multiple treatments they have had in multiple offices with every practitioner missing the desired target, it may be a sign of BDD and further treatment would serve no useful purpose for the patient and most likely misery for you.

Watch Them
One of the biggest clues to helping your patients is watching them while they are talking. Ask them anything. Ask them about their lives, what is coming up, what they are doing for the weekend, or what they are doing after they leave your office. Ask them why they have come to see you. As they talk, watch their movements and expressions. This is where nearly all of people’s issues come from.
We all make many faces that are unnecessary. They serve no purpose, yet we make these distortions that eventually define us, though often we are not happy with the resulting definition. Any treatment to the area would be short-lived, because their muscles are stronger than anything we can insert into their skin. The problem with these habitual faces is that once they become a habit, there is never a real break. They will make these faces during their sleep and treatment to fill the lines or deficits will not last as long as it could if they were more conscious of their movements.
Sleep Preference
Oftentimes someone will come in saying they had something done and the practitioner put “more on this side, so the other side looks worse.” Or, they will say that one side seems different than the other. This is normal. No one is totally symmetrical, and they would probably not look normal if they were. We continually show the effects of life the way we live it. If someone smokes, their skin tone will be pale, dry, wrinkled, and somewhat death-like. If they are complete sun worshippers, they will have bountiful issues including sunspots (age spots, liver-spots, etc.), seborrheic keratoses, extensive wrinkles, shiny, wax-like skin, and most likely precancerous lesions (depending upon age and damage severity). But even if they have none of these skin problems, after the age of 40, one side will be different than the other. This has much to do with not only fat, collagen, and bone loss, but the side they sleep on most, and many develop a stronger muscle pull on one side compared to the other.
Professional Familiarity
In a situation where patients want to enhance their desired outcomes, you will gain more from the experience (which translates to so much more for the patient) if you present yourself as a professional friend. This is not “pretend,” rather it is a real scenario. What you want to elicit is their current lifestyle, what they are doing, why they feel they need something, and where they want to go from here. Trying to understand where they are (it can take as few as 2 minutes) can make the difference between a keeper and a “never-see-again” patient.
One of the most valuable tools available, but too few practitioners perform is the action of “touch.” A quick touch of their arm when making a point in your conversation does wonders for creating a bond. You also can comment on their hair, or just do something, simply to familiarize yourself to them. It works. It takes away tension. These patients have tension because they know a needle is in their immediate future, and they do not know exactly how it will show up. Additionally, the medical assistant, if possible, can hold their hand if they see trepidation in their eyes. It also makes you feel like a friend, instead of a provider (think dentist).
Before You Start
Providing general medical care is difficult enough when it comes to patients following instructions and achieving a reasonable desired outcome. Compliance is typically an issue when dealing with such maladies as hypertension, diabetes, and hyperlipidemia, to name a few. It would always amaze me when I would see them back in 6 weeks only to tell me what they thought they had heard, which was often vastly different from what was prescribed. Memories of the visit and its subsequent details miraculously disappear.
While that type of memory deficit can be common among the general patient population, nothing will create fulminant amnesia like a cash-paying patient desiring cosmetic enhancement to build self-esteem. Suddenly flaws can appear that “were never there before” and of course are the result of the treatment that you provided. Or, the troublesome area they came to see you for is still troublesome, at least in their eyes. To this they say, “It did not work.” While it is sometimes possible that a neuromodulator for whatever reason may not have performed to their or even your satisfaction, there really is no way a “filler” cannot work. Unless it was placed so deeply that it became lost in the subcutaneous fat and is too deep to make a difference to the targeted deficit.
A bit more time should be spent when you sense that your patient is simply attempting to improve self-esteem. A good consult and a good conversation will leave your patient more satisfied, especially if they feel “heard.” It would benefit the practitioner, however, to point out that the issue the patient is complaining about can be addressed, but it may only result in a “fresher” or more rested look. It will not be a dramatic change that will change the outlook of the patient.
Worth a Thousand Words (and Your Protection)
Because these issues will appear, it is imperative to take pictures prior to the treatment. Ideally, sequential pictures starting with repose, then big smile (crow’s feet, bunny lines, and jelly-roll), frown (11s or 111s, bunny lines, horizontal crease between eyes), and finally quizzical brow lifting (forehead lines, degree of lifting of skin off of eyelids) will demonstrate what is going on before you ever get involved. This way, when someone comes back to you saying her crow’s feet are gone but now she has this “bulge” under her eyes that “she never had before” you can pull up the picture and say, “Yes, you had it, you just did not see it before because you were most likely concentrating on the crow’s feet. Once they were gone, you focused on other things.”
Showing your patients the before-treatment pictures in a situation like this most often puts all questions to rest. Sometimes it is necessary to take another picture after the treatment and do side by side comparison to completely illustrate the improvement. If they did not see it before, they should see it in a 2-dimensional comparison.
ANATOMY
The Integumentary System
The integumentary system includes the skin, hair, glands, nails, sensory receptors, and a vascular network. The skin is the largest organ of the body and covers more than 3000 square inches in the average adult. It makes up about 7% of total body weight. The lips, soles, and palms have no hair. The skin consists of 3 major layers: the epidermis, the dermis, and the subcutaneous tissue. The epidermis, more superficial than the dermis consists mostly of dead keratin cells. Melanin is a brown-black pigment produced from melanocytes and found mostly in the epidermis. People of all races have approximately the same number of melanocytes in the skin.6
The skin varies from each individual and also varies from one area of the body to another.7 The epidermis varies in thickness from .05 mm on the eyelids to approximately 1.5 mm on the palms and soles. Dermis thickness ranges from .03 mmon the eyelid to approximately 4 mm on the back.8,9
The Epidermis
The epidermis contains keratinocytes, which synthesize keratin, a protein with a protective role. The epidermis contains other cells including melanocytes, Langerhans cells, and Merkel cells. High concentrations of Merkel cells in areas such as the fingertips and the lips result in higher tactile resolution and sensitivity than other areas.10 The stratum corneum is the top layer of the epidermis and was once thought to be nothing more than a dead shroud of keratin cells with a main purpose of keeping things out and keeping things in. It has been studied by multiple disciplines that have revealed the stratum corneum to be a dynamic tissue with multiple functions.11 It has also been described as “bricks and mortar;” the corneocytes represent the bricks while the intercellular lipid bilayer signifies the mortar. The connotation of this representation, however, suggests something firm and immovable, where the actual stratum corneum is pliable, elastic, semi-permeable, and self-restoring.12 The basal layer contains basal cells, which have been termed the “stem cells” of the epidermis since they are undifferentiated proliferating cells. Daughter cells begin to rise from the basal layer and begin differentiation. It takes approximately 4 weeks for cells to migrate from the basal layer to the top of the stratum corneum where they are finally shed. Injury, inflammation, and certain treatments can speedup this process.9
The Dermis
The principle component of the dermis is collagen, which constitutes a family of fibrous proteins comprising at least 15 genetically distinct types in human skin. Collagen is the major structural protein for the entire body. It can be located in tendons, ligaments, lining of the bones, as well as the dermis. Collagen comprises 70% of the dry weight of skin.6 Collagen and elastic fibers are fibrous proteins that form the strong yet compliant skeletal matrix. In the uppermost part of the dermis (papillary dermis), collagen fibers are fine and loosely arranged. In the remainder of the dermis (reticular dermis), the fibers are thick and densely packed. Nerves and blood vessels are found in the dermis as the skin is a major sensory receptor. The nerve supply of the dermis is segmental, following dermatomes, with considerable overlap between segments.9
BOTULINUM TOXIN
Botulinum exotoxin is a polypeptide neurotoxin derived from the anaerobic bacterium Clostridium botulinum. It acts at the level of the neuroneal endplate, preventing the release of acetylcholine from the presynaptic neuron. The toxin produces a temporary chemical denervation causing weakness or a partial paralysis of striated muscle.13
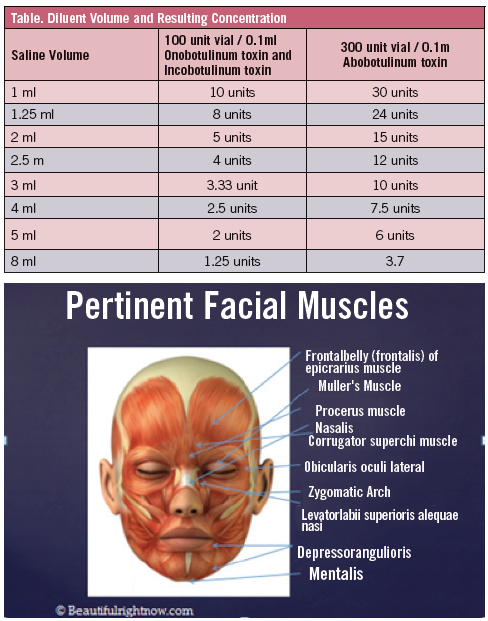
C botulinum toxins include 7 distinct serotypes, identified as A, B, C1, D, E, F, and G. These serotypes share the ability to block neurotransmission at the neuromuscular junction by blocking acetylcholine release, producing denervation and atrophy of cholinergic skeletal muscles. Because the neurotoxin serotypes differ in their cellular mechanisms of action and in the size of the neurotoxin complex, however, they are not interchangeable and their clinical profiles vary. Botulinum toxin type A (BTX-A) is the most powerful toxin and was the first to be developed for clinical use.14 BTX-A is distributed in a crystalline form. The package inserts on the 2 available in the United States recommend reconstitution with sterile, nonpreserved saline. More recent data, however, suggest that reconstitution with preserved saline does not impair the stability of BTX-A and is less painful than nonpreserved saline, due to the lower pH of the nonpreserved saline. The optimum concentration depends on the procedure. The Table outlines saline volume concenetrations. Research shows that most practitioners reconstitute with the recommended volume of 2.5 mL, yielding 4 units per 1 mL. Although the package inserts suggest that the reconstituted toxin should be used within 4 hours, evidence now indicates that the reconstituted product can be stored refrigerated for a week or longer without any loss of efficacy.14
Local injection of the toxin into selected muscle beds (Figure 1) has been used in various clinical situations for more than 3 decades. The first described use was for strabismus caused by ocular muscle spasticity. Since then, several other uses for the toxin have been described, including treatment of spastic muscle disorders, involuntary movement disorders, dystonias, muscle spasms, and autonomic disorders. In 1992, physicians Jean and Allistair Carruthers published their experience using botulinum toxin for improvement of periorbital rhytids. They noted incidental improvement in glabellar frown lines after treating patients for blepharospasm, which was the impetus behind exploring cosmetic uses for the toxin. Many articles subsequently were published describing various techniques for botulinum toxin use in rejuvenating the aging face and neck.15
Side effects that may occur with BTX-A injections include transient swelling or bruising at the injection site, mild headache, and flu-like symptoms. To minimize ecchymosis, patients are instructed to avoid aspirin, NSAIDs, and vitamin E. Ice application prior to injection may further minimize the risk of bruising.
BTX-A is contraindicated in patients with neuromuscular disease, such as myasthenia gravis and amyotrophic lateral sclerosis. Experience with BTX-A in pregnant and lactating women is extremely limited, so caution is warranted in these cases. Other contraindications include infection at the injection site, or a known hypersensitivity to any of the product contents. The possibility of drug interactions exists, and patients taking aminoglycoside antibiotics should receive smaller doses.14
Glabellar Treatment
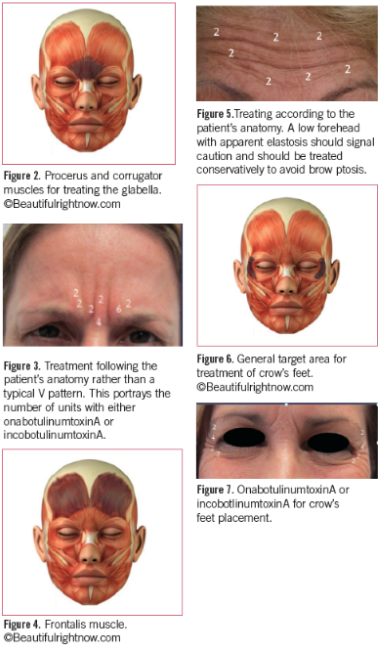
Since its FDA approval in 2002 for glabellar lines, the use of BTX-A has been well-studied and its clinical efficacy and safety profile have been established. Its efficacy is typically sustained for approximately 4 months though it can extend to 11 months in some patients.15 Figure 2 represents the muscle targeted for treating the glabella (shaded). It should be recognized, however, that there is often a great variability in the musculature of individuals.14,16,17
The dosage and placement are dependent upon the muscle strength, location, and size. Rather than simply placing the toxin according to a drawing in an article or label, it is best to have the patient animate as the muscle belly and size will be much more obvious. At this point, it is sometimes helpful to use a surgical marker to outline placement while the patient is animating (Figure 3). The average dosage for this site is 20 to 24 units for onabotulinum toxin type A and incobotulinum type A, and 50 to 60 units for abobotulinum toxin type A.
Frontalis Treatment
Currently, only approved for treatment in the glabella for cosmetic purposes, and onabotulinum toxin also for crow’s feet, treatment of forehead lines and targeting of the frontalis muscle is currently off-label.18
As with treatment of the glabella, the frontalis muscle varies from individual to individual (Figure 4). Careful assessment of the skin quality is also required to avoid sagging of thin skin due to lack of treated muscle pull and appearance of a brow ptosis (Figure 5). Brow ptosis is caused by diffusion of product into the frontalis either by excessive volume when injecting the glabella, or excessive manipulation after product injection. The sites should not be massaged and the patient is advised to remain upright for 4 hours to prevent undesired diffusion. Injection sites should be at least 1 cm above the bony rim and 1.5 cm laterally.19
Crow’s Feet
Crow’s feet in the lateral canthal area are produced by the action of the sphincteric orbicularis oculi, whose fibers are arranged in a circular pattern around the eyes, and also by the elevators of the corner of the mouth, risorius, and zygomaticus (Figure 6). Contraction of orbicularis is needed for forceful closure of the eyelids. The goal of treatment is to produce a weakening just in the area of the crow’s feet lines. Treatment of the lateral orbital (crow’s feet) areas with onabotulinumtoxinA produces satisfactory amelioration of wrinkling in this area. When treating this area it is important to treat only the area that shows wrinkling (Figure 7). In addressing the periocular area with botulinum toxin, it is possible to erase crow’s feet, soften lateral oblique lines on the forehead, smooth the inferior oblique lines of the cheek, soften the suborbital area, and elevate the lateral eyebrow.19
Care must be taken to avoid the zygomatic arch as this could result in an altered smile.
Botulinum toxin in the lower face should be reserved for the experienced clinician. Perioral rhytids become ubiquitous as one ages since the mouth is a sphinteric muscle. Many patients tend to blame it on smoking but the pucker is a natural face to make and many make it during pensive moments. Small doses (and I recommend diluting the toxin further by 50%), not more than 1 to 2 units (onabotulinumtoxinA and incobotulinumtoxinA) per quadrant is recommended.14 It may be divided up into several sites, however.
DERMAL FILLERS
HA fillers are used extensively in aesthetics today (Figure 8). Because the properties of HA fillers vary, their uses can vary also. The HA fillers are defined as gels because they consist of both a solid phase, suspended in a fluid phase. The viscosity and hardness of a gel depend upon their concentration of solid-phase molecules, the type and cross-linking, the molecular weight, and the gel to fluid ratio contained after manufacturing. Two rheological properties that can be measured and are important are its complex viscosity (η*) and its elastic modulus (G'). These properties help to determine how the filler behaves while being injected and after it is injected. How it flows is determined by the η* and its ability to retain its shape against the forces of skin pressure and movement is related to the G'.20
Molecular weight may also play a role in the choice of product. The molecular weight of HA has to do with the number of repeating disaccharides in the HA molecule. However, when applied to a filler, the cross-linking renders the final product molecular weight so enormous it cannot accurately be measured.21 Therefore, molecular weight in general may not be so much a factor but the final combination may be. For example, Juvéderm Voluma®, the newest HA in the Juvéderm family, is comprised of longer HA chains with high molecular weight and shorter HA chains with a lower molecular weight as well. Therefore, Voluma® intercollates between the tissues.22 This is one of the factors in its resistance to degradation.
The most common uses for HAs are nasolabial folds and marionette lines (Figure 9). Most HAs are approved for wrinkles and folds. All HAs are used extensively off-label in other areas for which they are not directly indicated but prove to be a very effective treatment for multiple issues. Calcium hydroxylapatite is a longer-lasting filler (longer than most HA fillers) comprised of calcium spheres surrounded by a carboxy-methylcellulose gel. As the gel is absorbed by the patient, the space is supposedly replaced with newly produced collagen. The ability to grow collagen is relative to the patients age, health, rate of metabolism, and area in which the product was placed.23
Poly-L-Lactic Acid
Poly-L-lactic acid (PLLA) is a biodegradable polymer of L-lactic acid. It has been used extensively in various applications for people for many decades. The PLLA molecule is heavy and irregularly shaped which contributes to its slow absorption. By 9 months, the particle is no longer detectable.24 The particle and its shape contributes to its ability to stimulate collagen growth. It has been approved in Europe since 1999 and now, has extensive use in many countries, including the United States. Originally approved for HIV-associated lipoatrophy, it has been used off-label cosmetically since 2004, and on-label cosmetically since 2009.
The use of PLLA has evolved from tissue-augmentation to foundational structure recovery. It is used to address the volume loss that leads to the appearance of aging (Figure 10). Volume loss includes loss of bone, fat, as well as loss of skin quality. As a biostimulatory agent, PLLA requires the host to react to it; therefore, the results may not be completely predictable, and are not immediate.25 With adequate consultation and information given to the patient, as well as reminding them that the results are not immediate, the outcome of PLLA can be amazing.

Adverse Events
The rate of complications among dermal fillers and aesthetic medicine is relatively low. This does not include plastic surgery. However, the main issues that people experience are injection pain, bruising at injection site, inflammation, swelling, and possible allergic reaction, which is rare. At one time bovine collagen was a filler with a rather high rate of allergy to the product. Bovine collagen is used today in Artefill®, a permanent filler and a skin test is required prior to injection.
There have been some reports of delayed hypersensitivity reaction to HA fillers. This may be due to bacterial impurities during the fermentation process.26 One report retrospectively reviewed HA reactions in patients worldwide. One out of 1400 developed hypersensitivity reaction with localized induration and swelling at the treatment site. There were no reports of systemic allergies.27 For these types of reactions, hyaluronidase may be used to break down the remaining HA.28
Vessel occlusion remains the most onerous of possible complications. However, it is estimated that perhaps some incidents of vessel occlusions may be due to a tamponade of the particular vessel, rather than direct vessel injection. Massage, heat, and perhaps nitropaste will be beneficial. Aspiration prior to any injection is also warranted.
References:
1.American Society for Aesthetic Plastic Surgery. The American Society for Aesthetic Plastic Surgery reports Americans spent the largetst amount on cosmetic surgery since the great recession. www.surgery.org/media/news-releases/the-american-society-for-
aesthetic-plastic-surgery-reports-americans-spent-largest-amount-on-cosmetic-surger.
Accessed July 13, 2014.
2.Mayo Clinic. Body dysmrphic disorder. www.mayoclinic.com/health/body-dysmorphic-disorder/DS00559/DSECTION=symptoms.
Accessed February 10, 2014.
3.Lewis W. The nuances of dealing with cosmetic patients. J Drugs Dermatol. 2004;3(1):67-70.
4.Petrou I. The successful aesthetic consult. Dermatology Times. January 30, 2014. http:dermatologytimes.modernmedicine.com/derm. Accessed February 10, 2014.
5.Oppenheimer RM, Fodor PB, eds. Be Your Best: A Comprehensive Guide to Aesthetic Plastic Surgery, Written by the Experts. Austin, TX: Insight International Press, LLC; 2006.
6.Odom RB, James WD, Berger TG. Diseases of the Skin. 9th ed. Philadelphia, PA: WB Saunders Company; 2000:6-7.
7.Gaboriau HP, Murakami CS. Skin anatomy and flap reconstruction. Otolaryngol Clin North Am. 2001;34(3):555-569.
8.Habif TP. Skin anatomy. In: Habif TP, ed. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. New York, NY: Elsevier; 2009:1.
9.Marks JG, Miller JJ. Structure and function of the skin. In: Marks JG, Miller JJ, eds. Lookingbill & Marks’ Priciples of Dermatology. 4th ed. Philadelphia, PA: Elsevier; 2006:5-7.
10.Kolarsick PA, Kolarsick MA, Goodwin C. Anatomy and physiology of the skin: erratum. J Dermatol Nurses Assoc. 2011;3(4):203-213.
11.Kligman AM. A brief history of how the dead stratum corneum became alive. In: Elias PM, Feingold KR, eds. Skin Barrier. New York, NY: Taylor & Francis; 2006:15-24.
12.Del Rosso JQ, Levin J. Clinical relevance of maintaining the structural and functional integrity of the stratum corneum: why is it important to you? J Drugs Dermatol.
2011;10(10 suppl):S5-S12.
13.Flynn TC, Carruthers JA, Carruthers JA. Botulinum-A toxin treatment of the lower eyelid improves infraorbital rhytides and widens the eye. Dermatol Surg. 2001;27(8):703-708.
14.Carruthers J, Carruthers A. Botulinum toxin A in the mid and lower face and neck. Dermatol Clin. 2004;22(2):151-158.
15.Fagien S, Cox SE, Finn JC, et al. Patient-reported outcomes with botulinum toxin type A treatment of glabellar rhytids: a double-blind, randomized, placebo-controlled study. Dermatol Surg. 2007;33(1 Spec No):S2-S9.
16.Lovice D. Botulinum toxin use in facial plastic surgery. Otolaryngol Clin North Am. 2002;35(1):171-186.
17.Carruthers JA, Lowe NJ, Menter MA, et al. A multicenter, double-blind, randomized, placebo-controlled study of the efficacy and safety of botulinum toxin type A in the treatment of glabellar lines. J Am Acad Dermatol. 2002;46(6):840-849.
18.Taub AF. Procedures offered in the medical spa environment. Dermatol Clin. 2008;26(3):341-358.
19.Carruthers J, Carruthers A. Botulinum toxin in facial rejuvenation: an update. Dermatol Clin. 2009;27(4):417-425.
20.Sundaram H, Voigts B, Beer K, Meland M. Comparison of the rheological properties of viscosity and elasticity in two categories of soft tissue fillers: calcium hydroxylapatite and hyaluronic acid. Dermatol Surg. 2010;36:1859-1865.
21.Kablik J, Monheit GD, Yu L, et al. Comparative physical properties of hyaluronic acid dermal fillers. Dermatol Surg. 2009;35(suppl 1):302-312.
22.Jesitus J. Filler lift a result of more that G prime. Dermatology Times. http://dermatologytimes.modernmedicine.com. Accessed May 23, 2014.
23.Pavici T. Calcium hydroxylapatite filler: an overview of safety and tolerability. J Drugs Dermatol. 2013;12(9):996-1002.
24.Rotunda AM, Narins RS. Poly-L-Lactic acid: a new dimension in soft tissue augmentation. Dermatol Ther. 2006;19(3):151-158.
25.Fitzgerald R, Vleggaar D. Facial volume restoration of the aging face with poly-l-lactic acid. Dermatol Ther. 2011;24(1):2-27.
26.Requena L, Requena C, Christensen l, et al. Adverse reactions to injectable soft tissue filler. J Am Acad Dermatol. 2011;64(1):1-34.
27.Monheit GD, Coleman, KM. Hyaluronic acid fillers. Dermatol Ther. 2006;19(3):141-150.
28.Brody HJ. Use of hyaluronidase in the treatment of granulomatous hyaluronic acid reactions or unwanted hyaluronic acid placement. Dermatol Surg. 2005;31(8 Pt 1):893-897.