
A Healthy Neonate With Chest Radiolucencies
A boy was born via unremarkable cesarean delivery to a 21-year-old primigravida following an uncomplicated pregnancy. Apgar scores were 8 at 1 minute and 9 at 5 minutes, and the boy’s birth weight was 3.345 kg.
On arrival at the well-baby nursery, his vital signs were within normal limits, and the only notable finding on physical examination was a nursing assessment of “absent heart sounds.”
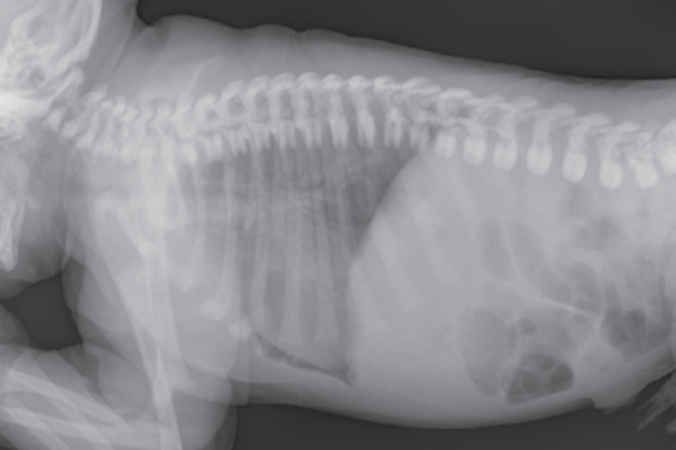 Lateral chest radiograph showed a prominent lucency in the anterior cardiophrenic angle (Figure 1). On anteroposterior radiograph, a small, thin rim of lucency was visible along the right heart border.
Lateral chest radiograph showed a prominent lucency in the anterior cardiophrenic angle (Figure 1). On anteroposterior radiograph, a small, thin rim of lucency was visible along the right heart border.
How do you read these images?
(Answer and discussion on next page)
ANSWER: Symptomless pneumopericardium
The radiographic lucent regions were thought to likely represent a small pneumopericardium. The infant was monitored closely in the nursery and remained asymptomatic. Follow-up echocardiography on day 3 showed normal parasternal and apical views, suggesting resolution of the pneumopericardium.
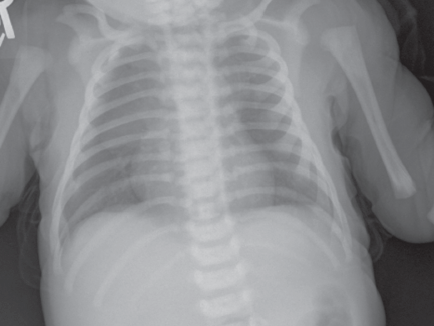
Figure 2. Anteroposterior radiograph showing a thin, lucent rim along the right heart border, consistent with a small pneumopericardium. No halo sign or continuous diaphragm sign is present, reflecting a minimal amount of air in the pericardial sac.
Neonatal pulmonary air-leak syndromes include pneumothorax, pneumomediastinum, and pneumopericardium; pneumopericardium is the rarest of the three,1 most often occurring in premature infants with respiratory distress syndrome.2
Cases of pneumopericardium in neonatal respiratory distress syndrome often are associated with other air leaks, such as pneumothorax or pulmonary interstitial emphysema, secondary to barotrauma from resuscitation or mechanical ventilation.3 Extra-alveolar air dissects along perivascular and peribronchial sheaths toward the mediastinal space (the Macklin effect) and enters the pericardial space at the reflection of the pericardium on the pulmonary vessels.4 However, pneumopericardium sometimes is an isolated finding without associated air-leak syndromes. In one reported neonatal case, pneumopericardium was related to a pericardial defect,5 but in other cases, the presence of anatomic abnormality could not be determined.2
The severity of pneumopericardium symptoms ranges from virtually asymptomatic with no hemodynamic compromise, as in this case, to tamponade-like symptoms with cardiac decompensation, desaturation, and death. Tension pneumopericardium is the most severe manifestation, with mortality rates reportedly as high as 83%.6 As far as we can determine, this could be the only reported case of a full-term infant with physical findings of pneumopericardium but who had no respiratory distress, who was not undergoing positive-pressure ventilation, and who had no hypotension, acidosis, cyanosis, pallor, or other symptoms of decreased cardiac output.
The diagnosis of pneumopericardium is confirmed with chest radiography: Anteroposterior view radiographs will show air surrounding the heart shadow (the halo sign) and outlining the superior border of the diaphragm (the continuous diaphragm sign).2
In tension pneumopericardium, the cardiothoracic ratio may be decreased, and the heart may appear slender.7 Electrocardiography findings, such as low voltages or small QRS complexes, appear to be inconsistent and unreliable.
In many cases of pneumopericardium, there is no time to perform these diagnostic studies. Therefore, in symptomatic infants with signs of tamponade (bradycardia, hypotension, increased respiratory distress, cyanosis, muffled heart sounds) and a suspicious history, emergent decompression by needle pericardial drainage is both diagnostic and therapeutic. Air reaccumulates in approximately 50% of pneumopericardium cases after initial aspiration; thus, a pericardial drainage tube also may be necessary.8 Asymptomatic patients may be observed closely with serial chest radiographs to confirm resolution of the pneumopericardium.9
References:
1.Trujillo MH, Fragachan CF, Tortoledo F. Cardiac tamponade due to pneumopericardium. Cardiology. 2006;105(1):34-36.
2.Burt TB, Lester PD. Neonatal pneumopericardium. Radiology. 1982;142(1):81-84.
3.Itani MH, Mikati MA. Early onset neonatal spontaneous pneumopericardium. J Med Liban. 1998;46(3):165-167.
4.Varano LA, Maisels MJ. Pneumopericardium in the newborn: diagnosis and pathogenesis. Pediatrics. 1974;53(6):941-945.
5.Siplovich L, Bar-Ziv J, Karplus M, Mares AJ. The pericardial “window”: a rare etiologic factor in neonatal pneumopericardium. J Pediatr. 1979;94(6):975-976.
6.Heckmann M, Lindner W, Pohlandt F. Tension pneumopericardium in a preterm infant without mechanical ventilation: a rare cause of cardiac arrest. Acta Paediatr. 1998;87(3):346-348.
7.Mirvis SE, Indeck M, Schorr RM, Diaconis JN. Posttraumatic tension pneumopericardium: the “small heart” sign. Radiology. 1986;158(3):663-669.
8.Reppert SM, Ment LR. The treatment of pneumopericardium in the newborn infant. J Pediatr. 1977;90(1):115-117.
9.Türkbay D. Pneumopericardium in a term infant on nasal continuous positive airway pressure (published correction appears in Arch Dis Child Fetal Neonatal Ed. 2007;92(4):F328). Arch Dis Child Fetal Neonatal Ed. 2007;92(3):F168.
Dr Brian J. Young is a pediatrician in Kenner, Louisiana. Dr Bronfin is a pediatricians and Dr Thomas Young is a pediatric cardiologist at the Ochsner Children’s Health Center in New Orleans, Louisiana.
William Yaakob, MD—Series Editor:Dr Yaakob is a radiologist in Tallahassee, Florida.