
Geriatric Dermatology: A Generational Approach
ABSTRACT: The most recent statistics predict that 1 in 5 people will be over the age of 65 by 2050. For the primary care practitioner, this means that older patients are a vital part of any medical practice. This article discusses the risk factors for skin disorders and offers treatment pearls when treating the geriatric population. A generational approach is designed to help optimize skin health over the course of a lifetime.
Geriatric dermatology is a rapidly growing field. Individuals age 65 and older now comprise 13.7% of the population in the United States, which amounts to roughly 1 in every 7 Americans. Since 2002, the number of individuals age 65 and older increased by 21% as compared to 7% for individuals under 65.1
Now totaling 43.1 million, this makes the 65 and older group the fastest growing age demographic in the United States. In addition, the older population itself is increasingly older. In 2012, the age 65 to 74 population (an estimated 24 million) was more than 10 times larger than in 1900, the age 75 to 84 group (an estimated 13.3 million) was 17 times larger, and the age 85+ group (an estimated 5.9 million) was 48 times larger. By 2050, 1 in 5 people will be age 65 or older (an estimated 88.6 million).1
The older patient is a vital part any medical practice. And, increased longevity will increase the number of elderly. As people live longer, their dermatologic needs will increase as the skin, hair, and nails must last longer. Dermatologists will increasingly focus on how the skin can optimally perform for a longer period.
Taking a Generational Approach
With several 40-year-old patients in my private practice, I took note to observe the changes in their skin over the next decade until they hit their 50s in 2004. Their sixth decade brought on more skin problems and these skin issues continue to present. Slowly, a pattern of skin aging emerged.2 Intervening where I could, I began to tease out the idea of looking at the aging process as an evolving process. My 65 and older geriatric patients did not turn 65 overnight. It happened 1 day, of 1 decade, at a time.
This prompted me to look at my 30-year-old patients with generational eyes—or anticipate the likely trajectory of the patient’s skin based on genetic predisposition, indicators on physical exam, and body environment. Armed with that knowledge, I could then design primary and secondary preventative medical strategies early enough to potentially change the outcome; this concept is known as tertiary prevention.3
The goal of generational dermatology is to optimize skin health over the course of a lifetime. When I noticed evolving dynamic rhytids and peeling photodamaged skin, I began an early intervention by injecting fillers and neurotoxins to reduce future precancers. For my elderly patients who had dry foot, mobility, and nail disorders, I would recommend pedicures and foot massages.
The key to this approach is full body skin examination for early intervention—to look for clues on future morbidity rather than waiting for the patient to present with a skin disorder. Most importantly, you must be aware of the risk factors for disorders in the geriatric population. This article discusses the risk factors and offers treatment pearls to help manage skin disorders among this patient population.
 Overview of Skincare Issues
Overview of Skincare Issues
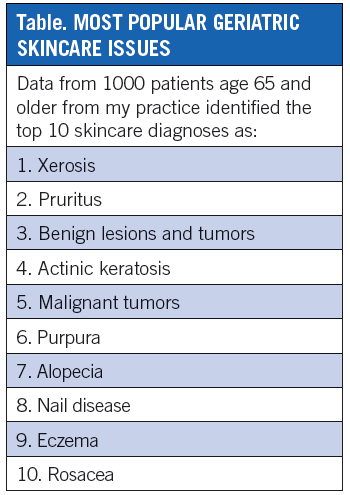
An internal practice survey polled 1000 patients (age 65 and older) to list the top 10 skincare diagnoses (Table), including xerosis, pruritus, rosacea, and eczema. In addition, rhytids, drug eruption, scabies, intertrigo, and folliculitis were well represented. These disorders occurred in men and women with equal frequency.4 A European retrospective study examining 2100 geriatric patients found similar results: the male to female ratio was 1.4 to 1 and the most common disorders were pruritus (18.9%), benign tumors (13.5%), actinic keratosis (9.1%), and malignant tumors (13.2%).5
Skin aging is a combination of chronologic (intrinsic) aging and environmental (extrinsic) aging.
Epidermal Changes of the Aging Skin Barrier
The stratum corneum, specifically the cornified envelope, is responsible for the barrier function of the skin. It is the outermost epidermal component and protects the skin from a harsh exterior environment. The cornified envelope is composed of a complex system of proteins and lipids. Aging skin has an extensively changed cornified envelope composition on the molecular level compared to young skin.6 There is downregulation of proteins filaggrin, loricrin, and late cornified envelope (LCE) 1 & 2 accompanied with marked up regulation of proteins SPRR-, S100-, and LCE3.
This knowledge is key in understanding the evolution of hyperkeratosis, ulcers, and wound characteristics in aged skin.6,7 Transepidermal water loss (TEWL) is an indicator for measuring healthy skin barrier function. TEWL in individuals 65 years and older has been found to be consistently lower when compared to a group of individuals age 18 to 64.8 Clinically, we need skincare strategies to prevent xerosis, pruritus, hyperkeratosis, and resultant ulcers in this older generation.
Kottner et al reviewed evidence-based skincare studies for maintaining skin barrier function and integrity in a 50-plus age group diagnosed with a dry skin condition, including dermatitis and superficial ulcerations. The reviewed studies had low levels of evidence. Skin-cleansing products containing syndets or amphoteric surfactants compared with standard soap and water washing improved skin dryness and demonstrated skin-protecting effects. Moisturizers containing humectants consistently showed statistically significant improvements in skin dryness. Skin barrier products containing occlusive reduced the occurrence of skin injuries compared with standard or no treatment.9
Conditions that may result from barrier function are numerous and include xerosis, which may preclude pruritus. Hyperkeratosis often seen in the elderly foot is the precursor to ulcers, as the faulty keratin cannot maintain integrity with trauma. Aesteatotic eczema and perineal irritant dermatitis occur secondary to decreased lipid content and a delayed barrier repair after skin irritation. Delayed barrier repair is caused by decreased enzymatic activity involved in lipid synthesis and processing, a changed cytokine profile, a less acid skin pH, and altered epidermal stem cell function.9,10
Xerosis Pearls For The Geriatric Patient
Here are treatment tips to review with geriatric patients presenting with xerosis:
• Environmental factors. Avoid cold temperatures, low humidity, and excessive water/washing
• Soap. Eliminate harsh and heavily fragranced soaps
• Water use. Limit skin contact to water to once daily for 10 minutes only.
• Cool it. Avoid hot water and instead use tepid or warm water
• Moisturize. This should be done 2 to 3 times per day—once after washing, plus 2 additional times daily Moisturizers rehydrate the corneocyets and promote structure of the diminishing lipid bilayer. Moisturizers hydrate the corneocytes. Urea, lactic acid, and glycerin attract and hold water. Occlusives can be layered over the moisturizer, petrolatum, mineral oil, coconut oil, and shea butter to prevent evaporation of the water decreasing TEWL in the severe xerotic.
• Corticosteroids. Severe aestheatotis, which has an inflammatory component (nummular dermatitis), can be treated with limited courses of mid-potency corticosteroids or calcineurin inhibitors that treat the inflammation, while moisturizers and occlusives work on barrier repair.9,10
Dermal Changes of Aging Skin Pearls
Dermal changes of aging skin are characterized by photodamage in response to oxidative stress, metalloproteinase, and
cytokine cascades.11 Heliodermatitis results in collagen and elastin degradation with change in shape and function of structural elements. Folliculosebaceous and eccrine structures decrease in size and production.
Resultant disorders are solar lentigines, telangiectasia, rosacea, purpura, stellate scars, benign neoplasms, actinic keratosis, skin cancer, fine rhytids, coarse rhytids, skin hypopigmentation and hyperpigmentation, alopecia, and sebaceous hyperplasia.
As individuals age, their skin undergoes dermal changes. Here are recommendations for older patients to help protect their aging skin:
• Sun protection and sun avoidance early in life.
• Avoid oxidative stressors (eg, smoking, alcohol, lack of sleep, diet).
• Eat a healthy diet of fresh fruits and vegetables that contain proven antioxidants including vitamin C, resveratrol, lycopene, beta-carotene, vitamin E, flavonoids, and lutein. Avoid high glycemic foods and grilled foods that contain polycyclic aromatic hydrocarbons.12
• Use cosmecuticals with evidence-based effects on skin.
• Consider intervention with skin resurfacing procedures, such as fractional lasers, medium depth chemical peels, photodynamic therapy, and cosmeceuticals that target collagen.11,13
Skin Cancer
Skin cancer is more frequently seen in older generations; evidence suggests that elder individuals have an increased susceptibility to nonmelanoma skin cancer (NMSC). Keratinocyte response to ultraviolet (UV) B irradiation is dependent on the activation of the insulin-like growth factor-1 receptor (IGF-1R) on them.14 IGF-1R is primarily activated by IGF-1 produced and secreted by papillary dermal fibroblasts. The expression of IGF-1 in the dermis diminishes with age due to an increase in senescent unproductive fibroblasts.15 Therefore, the skin of geriatric individuals is often deficient in IGF-1 leading to insufficient activation of the IGF-1R in geriatric epidermal keratinocytes.16
When exposed to UVB radiation, this IGF-1 deficiency results in an inappropriate response in epidermal keratinocytes that could permit the establishment of UVB-induced mutations in geriatric skin which then progress to NMSC.16 Clinical relevance is the observation that fractionated laser skin resurfacing was demonstrated to decrease the occurrence of senescent fibroblasts in geriatric dermis, increase the dermal expression of IGF-1 and correct the inappropriate UVB response.17
Skin cancer in the elderly may present a diagnostic challenge by atypical presentation and morphology. Basal cell carcinoma (BCC) may masquerade as telangiectasia, squamous cell carcinoma psoriasis, or a chronic nonhealing wound,18 and melanoma as a solar lentigo.
A full body skin history and examination identifying risk factors for skin cancer and lesions nonresponsive to prior therapies will lead to detection. Early detection promotes early nonsurgical or surgical treatment. Emerging noninvasive treatments of developing skin cancer include pharmacotherapy with 5-fluorouracil, imiquimod, diclofenac, ingenol mebutate, retinoids, and most recently topical application of the hedgehog pathway inhibitors. Vismodegib (Evivedge, Genentech USA, Inc.) is the first oral agent to treat BCC.19 Photodynamic therapy and radiation therapy may be effective. Invasive treatments include cryotherapy for actinic keratoses, desiccation, and curettage for superficial NMSC lesions, standard excision, and Mohs micrographic surgery.20
Skin Cancer Pearls For The Geriatric Patient
Here are strategies for the management and treatment of elderly patients with skin cancer:
• Continuing education in sun protection (eg, SPF, hats, sleeves, collars, eyewear, pants, shade seeking behavior).
• Patients with skin cancer risk factors may benefit from intervention by chemical peeling or fractionated carbon dioxide laser to prevent aging associated NMSC.13,21
• Histopathology can direct the course of treatment. A biopsied superficial BCC may not require excision but pharmacotherapy.
• Screen elderly skin cancer history patients 2 to 4 times per year for early detection.
• Vitamin D recommendations for the aging population: Maintain serum 25-(OH)-vitamin D3 levels in the 75 nmol/L to 100 nmol/L range.
An oral cholecalciferol intake of approximately 2000 IU/day is recommended as a supplement throughout the year for those who cannot enjoy the sun in summer or only during winter for others.22
Hair
Hair aging comprises decrease in hair pigmentation (graying) and decrease in hair production (alopecia). The scalp and hair are subject to intrinsic/chronologic aging, and extrinsic aging due to environmental factors, which include UV radiation, smoking, and nutrition.23 Evidence is emerging that androgenetic alopecia may be considered a form of organ-specific premature aging and associated with endocrine and cardiovascular morbidity.24,25
Hair Pearls For The Geriatric Patient
Keep the following tips in mind in treating elderly patients presenting with hair issues:
• Determine the type of hair abnormality.
• Consider intrinsic/genetic factors.
• Review environmental factors, such as comorbidities, diet, and nutrition. Oral supplements, such as biotin and marine fish extract, have controlled studies showing benefit.26 Selenium and keratin may have a role in hair health but lack controlled studies.26,27 Malnutrition is a known risk factor for alopecia.
• Female and male pattern hair loss may be associated with increased body mass index and associated increased risk for cardiovascular disease; therefore, complete physical exams are recommended.24,25
• Tailor treatment to adjust as many causative factors as possible. For example, topical minoxidil 5% with oral finasteride 1 mg and biotin.27
Nails
Nail disorders comprise approximately 10% of all dermatologic conditions. The lower extremity represents the second most common site of skin lesions in geriatric patients. Nail disorders are common in elderly patients. Onychodystrophies frequently observed in elderly patients reflect changes in color, shape, growth, thickness, and histology.28,29
Brittle nail syndrome (BNS) can result from a multitude of causes including advanced aging, poor nutrition, and medical comorbidities. They are characterized by soft, dry, easily breakable nails that show onychorrhexis (longitudinal splitting) and onychoschizia
(lamellar peeling).28,29
BNS has been shown to improve after supplementation with a 2.5 mg dose of biotin daily or a 10 mg dose of silicon daily.30,31
Nail fungal infections account for 50% of all nail disorders. It is reported at 40% in elderly subjects. However, it is probably higher because it is a disorder often undetected by healthcare professionals. Causes of onychomycosis include a reduced rate of nail plate growth with advancing age, change in keratin structure, decreased immune system, concomitant disease (eg, diabetes mellitus and peripheral arterial disease), nail trauma due to faulty biomechanics, immobility, and decreased foot care and nail clipping.28,29
Emerging Trends and Issues
Drug eruptions and pharmacotherapy polypharmacy of older patients may contribute to drug eruptions and coexisting skin conditions of xerosis and pruritus. Pharmacotherapy is an emerging critical subject for all geriatricians.32 Age-related physiologic changes and disease-related changes in organ function affect drug handling (pharmacokinetics) and response (pharmacodynamics). Multiple comorbidities, multiple medications (prescription, over-the-counter, homeopathic, supplements, and herbs), and multiple providers (prescribers, pharmacies, naturopaths, and internists) can contribute to this issue. In addition, this is compounded by the aging cognitive impairment, memory challenges and functional difficulties.32,33
The geriatric patient is your next cosmetic patient. During the full body skin examination, review the pathophysiology and therapeutic aspects of both aesthetic and medical disorders with the patient, including mid-face volume loss, dynamic and nondynamic rhytids, on and off face skin rejuvenation, and vein treatments. Also review best skincare practices and the role of cosmeceuticals as this is all a part of the aging patient.
The 65 and older patient is a rapidly growing demographic with unique skin, hair, and nail issues. Skin barrier is a significant issue creating the backdrop for conditions, such as xerosis, pruritus, and purpura. Emerging science suggests that photodamage and possibly even NMSC may be ameliorated with laser- and light-based technology. Hair disorders and alopecia may be associated with underlying comorbidities of an endocrine and cardiovascular nature. Skin cancer treatment modalities are becoming less invasive with new topical pharmacotherapeutics to treat early malignancies.
While nail disorders are often unrecognized, they may be prevented by encouraging foot health and hygiene. Polypharmacy plays an increasing role in drug eruptions and skin conditions. Practitioners need an understanding of drug metabolism and skin interactions.
In addition, cosmetic dermatology is increasingly becoming part of the culture for men and women as patients are living longer and want their skin to reflect their attitude not their age. Using a generational preventive approach toward the evolving aging patient can help target morbidity and guide patients toward best practices in putting their best skin forward during their golden years.
Disclosure: The author reports no relevant financial relationships. She has consulted for Allergan, Colore Science, L’Oreal, MELA Sciences, Neostrata, Skin Medica, Theraplex, Top MD, Valeant, and Viviviscal.
This article was originally published in the October issue of The Dermatologist.
References:
1. US Administration on Aging. The older population. www.aoa.gov/AoARoot/Aging_Statistics/Profile/2013/3.aspx. Accessed September 22, 2014.
2. Roberts WE. Generational dermatology: model of prevention and multi-decade approach to the evolving aging patient. J Drugs Dermatol. 2013;12(12):1396-1397.
3. Leavell HR, Clark EG. Preventive Medicine for the Doctor in his Community: An Epidemiologic Approach. 3rd ed. Huntington, NY: Robert E. Krieger Publishing Company; 1979.
4. In house data. Roberts WE.
5. Rubegni P, Poggiali S, Nami N, et al. Skin diseases in geriatric patients: our experience from a public skin outpatient clinic in Siena. G Ital Dermatol Venereol. 2012;147(6):631-666.
6. Rinnerthaler M, Duschl J, Steinbacher P, et al. Age-related changes in the composition of the cornified envelope in human skin. Exp Dermatol. 2013;22(5):329-335.
7. Seyfarth F, Schliemann S, Antonov D, Elsner P. Dry skin, barrier function, and irritant contact dermatitis in the elderly. Clin Dermatol. 2011;
29(1):31-36.
8. Kottner J, Lichterfeld A, Blume-Peytavi U. Transepidermal water loss in young and aged healthy humans: a systematic review and meta-analysis. Arch Dermatol Res. 2013;305(4):315-323.
9. Kottner J, Lichterfeld A, Blume-Peytavi U. Maintaining skin integrity in the aged: a systematic review. Br J Dermatol. 2013;169(3):528-542.
10. Kottner J, Lichterfeld A, Blume-Peytavi U, Kuhlmey A. Skin health promotion in the elderly. Z Gerontol Geriatr. 2014 Mar 1 [epub ahead of print].
11. Han A, Chien AL, Kang S. Photoaging. Dermatol Clin. 2014;32(3):291-299.
12. Katta R, Desai SP. Diet and dermatology: the role of dietary intervention in skin disease. J Clin Aesthet Dermatol. 2014;7(7):46-51.
13. Kubiak M, Mucha P, Debowska R, Rotsztejn H. Evaluation of 70% glycolic peels versus 15% trichloroacetic peels for the treatment of photodamaged facial skin in aging women. Dermatol Surg. 2014;40(8):883-891.
14. Kuhn C, Kumar M, Hurwitz SA, et al. Activation of the insulin-like growth factor-1 receptor promotes the survival of human keratinocytes following ultraviolet B irradiation. Intl J Cancer. 1999;80(3):431-438.
15. Lewis DA, Travers JB, Spandau DF. A new paradigm for the role of aging in the development of skin cancer. J Invest Dermatol. 2009;129(3):
787-791.
16. Lewis DA, Travers JB, Spandau DF. Aging-associated non-melanoma skin cancer: a role for the dermis. In: Farage MA, Miller KW, Maibach HI, eds. Textbook of Aging Skin. New York, NY: Springer; 2010:587-599.
17. Spandau DF, Lewis DA, Somani AK, Travers JB. Fractionated laser resurfacing corrects the inappropriate UVB response in geriatric skin. J Invest Dermatol. 2012;132(6):1591-1596.
18. Dewberry C, Norman RA. Skin cancer in the elderly. Dermatol Clin. 2004;22(1):93-96.
19. Clark CM, Furniss M, Mackay-Wiggan JM. Basal cell carcinoma: an evidence-based treatment update. Am J Clin Dermatol. 2014;15(3):197-216.
20. Berking C, Hauschild A, Kölbl O, et al. Basal cell carcinoma-treatments for the commonest skin cancer. Dtsch Arztebl Int. 2014;111(22):
389-395.
21. Micali G, Lacarrubba F, Nasca MR, Schwartz RA. Topical pharmacotherapy for skin cancer: part I. Pharmacology. J Am Acad Dermatol. 2014;70(6):
965.e1-e12.
22. Glossman H. Vitamin D, UV, and skin cancer in the elderly: to expose or not to expose? Gerontology. 2011;57(4):350-353.
23. Trüeb, R. Oxidative stress in ageing of hair. Int J Trichology. 2009;1(1):6-14.
24. Christoffersen M, Frikke-Schmidt R, Schnohr P, et al. Visible age-related signs and risk of ischemic heart disease in the general population: a prospective cohort study. Circulation. 2014;129(9):990-998.
25. Yang CC, Hsieh FN, Lin LY, et al. Higher body mass index is associated with greater severity of alopecia in men with male-pattern androgenetic alopecia in Taiwan: a cross-sectional study. J Am Acad Dermatol. 2014;70(2):297-302.e1.
26. Glynis A. A double-blind, placebo-controlled study evaluating the efficacy of an oral supplement in women with self-perceived thinning hair. J Clin Aesthet Dermatol. 2012;5(11):28-34.
27. Atanaskova Mesinkovska N, Bergfeld WF. Hair: what is new in diagnosis and management? Female pattern hair loss update: diagnosis and treatment. Dermatol Clin. 2013;31(1):119-127.
28. Cohen PR, Scher RK. Geriatric nail disorders: diagnosis and treatment. J Am Acad Dermatol. 1992;26(4):521-531.
29. Singh G, Haneef NS, Uday A. Nail changes and disorders among the elderly. Indian J Dermatol Venereol Leprol. 2005;71(6):386-392.
30. Cashman MW, Sloan SB. Nutrition and nail disease. Clin Dermatol. 2010;28(4):420-425.
31. Scheinfeld N, Dahdah MJ, Scher R. Vitamins and minerals: their role in nail health and disease. J Drugs Dermatol. 2007;6(8):782-787.
32. Boparai MK, Korc-Grodzicki B. Prescribing for older adults. Mt Sinai J Med. 2011;78(4):613-626.
33. Endo JO, Wong JW, Norman RA, Chang AL. Geriatric dermatology: Part I. Geriatric pharmacology for the dermatologist. J Am Acad Dermatol. 2013;68(4):521.e1-10.