
Peer Reviewed
Desquamating Rash and Facial Swelling in an Infant
A previously healthy 7-month-old boy presented with a 2-day history of a worsening generalized rash. Two weeks before presentation, he had sustained an abrasion to his right upper arm. The cause of the abrasion was unknown, but it had worsened and become weepy. He had also developed a fever that had lasted for 2 days and had a maximum temperature of 39.4°C. The fever resolved with ibuprofen, and the abrasion appeared to dry and heal 2 days prior to presentation.
However, the boy’s mother had noticed that his back, thighs, and occiput had several large blisters that easily ruptured. The patient’s 1 year-old sibling had had similar skin blisters that had resolved without sequelae. In addition, the patient’s mother reported that the patient had a red rash in the diaper area, with painful peeling in some regions. The boy was reported as being irritable but consolable.
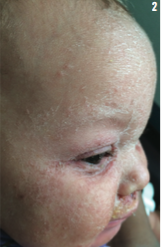
At presentation, the infant was also fussy but consolable. He had a mild cough and clear rhinorrhea, but he exhibited no respiratory distress, drooling, or difficulty swallowing. His eyes were not red, and he was afebrile. The boy’s vital signs were unremarkable, but physical examination results showed a diffuse, erythematous rash over the face, which extended to the scalp and ears. He had crusting over the eyelids and around the mouth and nose, with mild swelling concentrated in the orofacial region (Figures 1 and 2). There were yellow-crusted scabs with mild bleeding under the nares. Circular, hyperpigmented lesions were noted on the occiput, posterior trunk, right thigh, and right arm (Figure 3) with mild surrounding erythema. The lesions in these areas varied in size from 2 to 3 cm, and the skin within these lesions was thickened and scaly, with areas of weeping and purulent discharge.
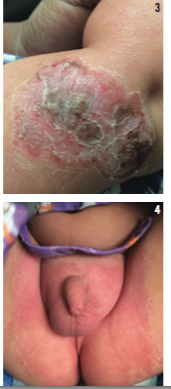
Additionally, there was erythematous, denuded skin around the perineum, extending around the penis, scrotum, and anus (Figure 4). The skin throughout the boy’s body appeared flushed. The oral and rectal mucosa were not involved. He had a negative Nikolsky sign, but there were sheets of peeled epidermis at the time of presentation, especially in the diaper area, where there could be the type of shearing force required to separate superficial epidermis seen with a Nikolsky sign. The rest of the physical examination results were unremarkable.

Why does this boy have a worsening, generalized rash?
(Answer and discussion are on the next page.)
Answer: Staphylococcal scalded skin syndrome
A presumptive diagnosis of staphylococcal scalded skin syndrome (SSSS) was made, and the patient was started on intravenous clindamycin 40 mg/kg/day every 6 hours. Staphylococcus aureus remains the most common cause of skin and soft tissue infections, with phage group II strains (Types 3A, 3B, 3C, 55, or 71) producing exfoliatins A and B, serine proteases selectively targeting desmoglein 1, an adhesion molecule within desmosomes in the stratum granulosa. Subsequent cell separation clinically manifests as flaccid blisters that slough off, leaving the underlying skin erythematous and denuded, which is the characteristic appearance of the skin (ie, scalded).1-4 Risk factors for developing SSSS include age, socioeconomic factors, overcrowding, azotemia, immunosuppression, viral infections, and antibiotic use. The most significant risk factor is disruption of intact skin. Children under 5 years of age, especially infants and newborns, are at an increased risk for SSSS due to insufficient time to develop specific lifelong antibodies to staphylococcal toxins and immature renal clearance. However, the prognosis in children is good relative to adults.3,4
DIAGNOSIS AND TREATMENT
Diagnosis of SSSS is usually made on the basis of the characteristic history and physical findings. Additionally, a skin biopsy can provide histologic confirmation of localization of the pathology in the zona granulosa.
Gram stain and cultures from blisters and wound sites do not typically yield any organism because there is hematogenous spread of toxins to distal noninfected sites. Isolation of the organism from sites of colonization, like the nasopharynx, has a better yield.2
Management of SSSS often includes parenteral antibiotic coverage to target S aureus, as well as supportive care measures such as fluid and electrolyte replacement. Increasing rates of community-acquired methicillin-resistant S aureus infection (MRSA) are an important consideration in antimicrobial therapy. If MRSA is suspected, antibiotics with MRSA coverage (eg, clindamycin, vancomycin, or linezolid) are indicated.5-9
In patients with recurrent skin and soft tissue infections due to S aureus, decolonization of the organism may be considered. In addition to general hygiene measures, these patients may undergo a decolonization regimen that could include nasal mupirocin twice daily for 5 to 10 days and a topical skin antiseptic solution (eg, chlorhexidine or dilute bleach baths) for 5 to14 days.10 Household members may also undergo decolonization with a skin antiseptic in an effort to reduce household transmission.
The patient described in the case had a desquamative rash with denuded areas of the skin. Bacterial culture from the anterior nares yielded methicillin-susceptible S aureus. Clinical improvement on intravenous clindamycin was significant after 2 days. The patient was discharged on oral clindamycin to complete a total of 10 days of antimicrobial therapy.
Uche Nwokidu-Aderibigbe, MD; Andrea L. Buenrostro, MD; and Rita Shah MD, are from the University of Nevada School of Medicine in Reno.
References
1. Handler MZ, Schwartz RA. Staphylococcal scalded skin syndrome: diagnosis and management in children and adults. J Eur Acad Dermatol Venereol. 2014;28(11):1418-1423.
2. Hubiche T, Bes M, Roudiere L, Langlaude F, Etienne J, Del Giudice P. Mild staphylococcal scalded skin syndrome: an underdiagnosed clinical disorder. Br J Dermatol. 2012;166(1):213-215.
3. Amagai M, Yamaguchi T, Hanakawa Y, Nishifuji K, Sugai M, Stanley JR. Staphylococcal exfoliative toxin B specifically cleaves desmoglein 1.
J Invest Dermatol. 2002;118(5):845-850.
4. Hanakawa Y, Stanley JR. Mechanisms of blister formation by staphylococcal toxins. J Biochem. 2004;136(6):747-750.
5. Acland KM, Darvay A, Griffin C, Aali SA, Russell-Jones R. Staphylococcal scalded skin syndrome in an adult associated with methicillin-resistant Staphylococcus aureus. Br J Dermatol. 1999;140(3):518-520..
6. Ito Y, Funabashi Yoh M, Toda K, Shimazaki M, Nakamura T, Morita E. Staphylococcal scalded-skin syndrome in an adult due to methicillin-resistant Staphylococcus aureus. J Infect Chemother. 2002;8(3):
256-261.
7. Noguchi N, Nakaminami H, Nishijima S, Kurokawa I, So H, Sasatsu M. Antimicrobial agent of susceptibilities and antiseptic resistance gene distribution among methicillin-resistant Staphylococcus aureus isolates from patients with impetigo and staphylococcal scalded skin syndrome.
J Clin Microbiol. 2006;44(6):2119-2225.
8. Kaplan SL, Deville JG, Yogev R, et al. Linezolid versus vancomycin for treatment of resistant Gram-positive infections in children. Pediatr Infect Dis J. 2003;22(8):677-686.
9. Kimberlin DW, Brady MT, Jackson MA, Long SS. Staphylococcal infections. In: Kimberlain DW, Brady MT, Jackson MA, Long SL, eds. American Academy of Pediatrics Red Book. 30th ed. Elks Grove Village, IL: American Academy of Pediatrics; 2015:715.
10. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52(3):e18-e55.