
Cupping and Coining: Alternative Medicine Delaying Myocardial Infarction Therapy
A 50-year-old Vietnamese man presented to the emergency department with a complaint of 3 days of progressively worsening, intermittent chest pain. He had a history of hypertension and recently had been started on combination lisinopril-hydrochlorothiazide but otherwise had no cardiac risk factors.
On presentation, physical examination findings were remarkable only for 2 well-circumscribed, circular ecchymoses over his right chest wall (Figure 1). When questioned, he reported having recently undergone treatment for his chest pain with cupping from a natural healer.

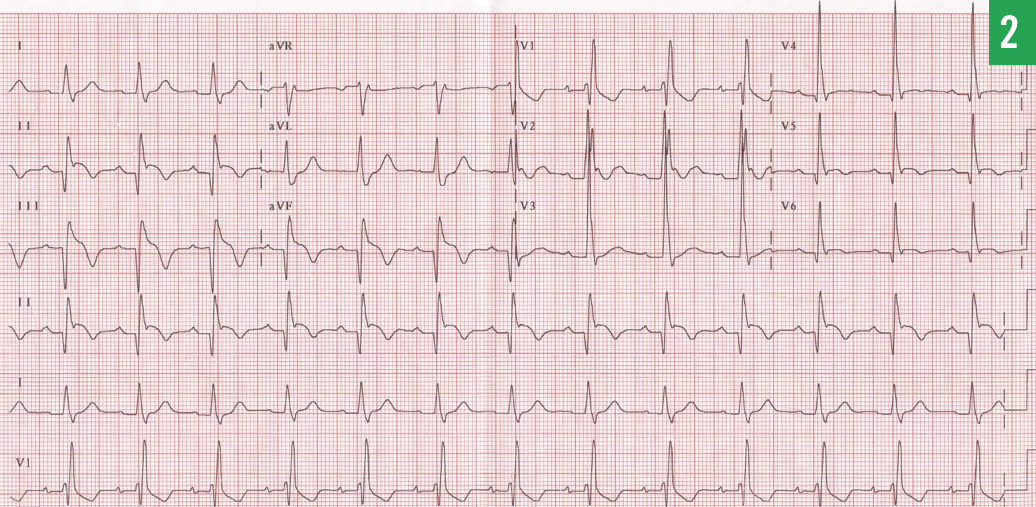
A 12-lead electrocardiogram (ECG) showed a recent inferolateral infarct pattern (Figure 2). Given his ongoing chest pain, he was taken to the cardiac catheterization laboratory, and a bare metal stent was placed to an occluded distal, dominant right coronary artery. His initial troponin I level was 32.1 ng/mL (reference range, < 0.05 ng/mL). His course was complicated by transient third-degree atrioventricular block and cardiogenic shock, but ultimately he recovered and was discharged.
In a second, unrelated case, a 75-year-old Cambodian man presented to the emergency department with chest pain, abdominal pain, nausea, and vomiting that had begun in the middle of the previous night. Physical examination revealed broad, linear hyperemic skin markings in a symmetric distribution across his chest and upper abdomen (Figure 3). He reported initially having sought treatment from a natural healer for his symptoms, and he had undergone coining without resolution of his pain.


The patient’s 12-lead ECG revealed a recent anteroseptal infarct pattern with lateral involvement (Figure 4). During emergent cardiac catheterization, a bare metal stent was placed to a 100% occluded mid-left anterior descending artery. His initial troponin T level was 1.2 ng/mL (reference range, < 0.01 ng/mL). The patient recovered well.
Discussion
Cupping is a traditional Chinese therapy that has been in use for more than 2000 years and is now practiced in numerous cultures. During cupping, air is heated briefly inside a glass cup, which is then placed onto the skin. As the air inside the cup cools, a vacuum effect results in a local area of ecchymosis. Wet cupping involves the addition of a small incision in the skin before the cup is placed.1
In his historic text, The Principles and Practice of Medicine, William Osler advocated cupping for treatment of bronchopneumonia and acute myelitis.2 From a cardiovascular standpoint, observations made from cupping led to the discovery of nitrates as antianginal agents in 1867. Thomas Lauder Brunton observed that “small bleedings of three to four ounces,” among other effects, served to lower blood pressure.3 He extrapolated that amyl nitrate would have similar efficacy. One contemporary report even suggests an improvement in angina symptoms and ECG abnormalities with cupping.4
Coining is another alternative medicine practice, prevalent in Southeast Asia, which consists of rubbing a coin, jade, or buffalo horn over lubricated skin. It is postulated that coining affects superficial blood flow and removes “heatiness” or “negative energies” through the skin.5 As a result, it is classically applied in attempts to relieve fever.
Coining is believed by healers to be more efficacious if more ecchymoses are created. Therefore, a treatment failure may be interpreted as an insufficient trial of therapy.5 This may provoke severe burns, with 1 case report documenting a 22% body surface area burn requiring a 10-day hospital stay.6
To health care providers who are unfamiliar with the practice of cupping or coining, the resulting ecchymoses may be misinterpreted as signs of abuse.7 Patients such as ours, who subsequently received coronary artery stents and thus required dual antiplatelet therapy, or patients on anticoagulation should be warned to avoid these therapies.5
Perhaps the greatest risk of cupping and coining are the delay in treatment of emergent conditions requiring immediate intervention, such as acute myocardial infarction. Patients who experience delays in percutaneous coronary intervention are shown to have a larger infarct size, lower ejection fractions at 6 months, and higher mortality at 1 year than patients who are treated earlier.8,9
Cupping and coining fall under the rubric of complementary and alternative medicine (CAM), other examples of which include acupuncture, meditation, and herbal supplements. Up to 40% of patients in the United States will utilize these methods each year.10 Health care providers thus should be aware of the use of alternative therapies and routinely question patients about it. Although CAM may have some benefit in the correct setting, it carries significant risk of adverse effects, and its implementation may delay the evaluation and treatment of life-threatening conditions that have proven medical therapies.
Gregary D. Marhefka, MD, is the associate director of the Cardiovascular Intensive Care Unit and an associate professor of medicine in the Department of Medicine, Division of Cardiology, at the Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia, Pennsylvania.
Andrew W. Panakos, MD, is a cardiovascular disease fellow at Jackson Memorial Hospital at the University of Miami in Miami, Florida.
Michael P. Savage, MD, is director of the angioplasty center and the cardiac catheterization laboratory at Thomas Jefferson University Hospitals and is the Ralph J. Roberts Professor of Cardiology at the Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia.
References:
- Cao H, Li X, Liu J. An updated review of the efficacy of cupping therapy. PLoS ONE. 2012;7(2):e31793.
- Osler W. The Principles and Practice of Medicine: Designed for the Use of Practitioners and Students of Medicine. McRae T, ed. 11th ed. New York, NY: D Appleton & Co; 1931:112, 981.
- Brunton TL. On the use of nitrite of amyl in angina pectoris. Lancet. 1867;90(2291):97-98.
- Lan Z, Gao ZW. Effective therapy for coronary artery disease using combined moxibustion, cupping and Chinese herbal plasters: report on 35 cases. Am J Acupunct. 1996;24(1):11-18.
- Tan AK, Mallika PS. Coining: an ancient treatment widely practiced among Asians. Malays Fam Physician. 2011;6(2-3):97-98.
- Amshel CE, Caruso DM. Vietnamese “coining”: a burn case report and literature review. J Burn Care Rehabil. 2000;21(2):112-114.
- Davis RE. Cultural health care or child abuse? The Southeast Asian practice of cao gio. J Am Acad Nurse Pract. 2000;12(3):89-95.
- Liem AL, van ‘t Hof AWJ, Hoorntje JCA, de Boer M-J, Suryapranata H, Zijlstra F. Influence of treatment delay on infarct size and clinical outcome in patients with acute myocardial infarction treated with primary angioplasty. J Am Coll Cardiol. 1998;32(3):629-633.
- De Luca G, Suryapranata H, Ottervanger JP, Antman EM. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation. 2004;109(10):1223-1225.
- Lin MC, Nahin R, Gershwin ME, Longhurst JC, Wu KK. State of complementary and alternative medicine in cardiovascular, lung, and blood research: executive summary of a workshop. Circulation. 2001;103(16):2038-2041.