
A Collection of Women’s Health Issues
Mucinous Cystadenoma
John M. Nakayama, MS, and Jinichi Tokeshi, MD
A 53-year-old perimenopausal woman presented to the emergency department with throbbing lower abdominal pain and distention. The pain started 5 days earlier and worsened with sitting and walking; she also experienced increasing dyspnea. She noticed increasing abdominal girth about 5 months earlier. Since then, she gained 5 lbs to 10 lbs, despite dieting
History. The patient reported a 22-pack-per-year history of smoking but no alcohol use. She was taking over-the-counter painkillers and allergy medications. Her family history was notable for a brother who died of laryngeal cancer.
Physical examination. The patient was 4 ft and 9 in, and weighed 115 lbs (normal weight: 105 lbs). Blood pressure was 148/72 mm Hg; other vital signs were normal. The abdomen was soft, distended, and tender without rebound or guarding; bowel sounds were normal. A palpable mass extended from thesymphysis pubis to near the umbilicus.
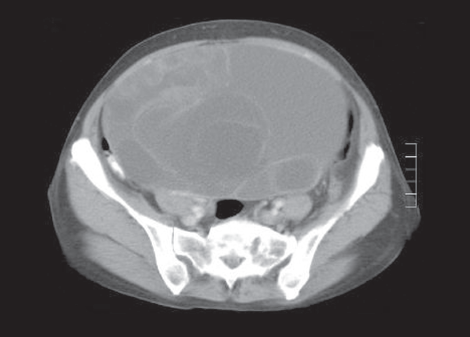
Laboratory testing. Results of a complete blood cell count, basic metabolic panel, urinalysis, amylase and lipase tests, and liver function tests were normal. A human chorionic gonadotropin urine test was negative. Abdominal and pelvic CT scans showed a large multiloculated cystic mass that arose from the pelvis and extended to the level of the diaphragm. There were multiple fibroids in the uterus and no peritoneal free fluid.
The cancer antigen 125 test (CA-125) value was 16 U/mL (normal range, less than 35 U/mL). Exploratory laparotomy revealed a large solid, cystic mass arising from the right ovary. A total abdominal hysterectomy and bilateral salpingo-oophorectomy were performed. The excised mass was 24 cm x 15 cm x 14 cm and weighed about 8 lbs; it was smooth without excrescences and was composed of gelatinous cysts. Pathological results revealed benign mucinous cystadenoma.
Discussion. Mucinous cystadenomas are relatively common (12%-15% of all ovarian tumors).1 They can become massive. These tumors usually develop in the third to fifth decades of life and typically cause vague symptoms, such as increasing abdominal girth, abdominal or pelvic pain, emesis, fatigue, indigestion, constipation, and urinary incontinence.2,3 Because this patient’s 8 lb tumor was disproportionately large for her small frame, it restricted the motion of her diaphragm and led to dyspnea.
Although mucinous cystadenomas are benign, they can progress to cystadenocarcinomas; they may also contain pockets of malignancy that are easily missed.4 Smoking is a known risk factor for mucinous ovarian cancer.5
Because the clinical picture of benign and malignant mucinous tumors is very similar, biopsy is the preferred method of diagnosis. Laparoscopy with characteristic ultrasonographic findings at a minimum is required; however, open laparotomy may be necessary for staging and treatment.6 Measurement of CA-125 is often not helpful for diagnosis, because an elevated level is an inconsistent finding in ovarian malignancies.
Diagnosis is often delayed because women frequently fail to report symptoms or attribute them to other causes (eg, menopause). This patient thought she was “getting fat” and ignored her symptoms until the tumor had grown significantly. Fortunately, malignancy did not develop during the 5-month gap between the first symptoms and diagnosis.
Outcome of the case. The patient tolerated the surgery well and recovered without complications. After the operation, she returned to her normal level of activity.
References:
1. Rodríguez IM, Prat J. Mucinous tumors of the ovary: a clinicopathologic analysis of 75 borderline tumors (of intestinal type) and carcinomas. Am J Surg Pathol. 2002;26(2):139-152.
2. Bankhead CR, Kehoe ST, Austoker J. Symptoms associated with diagnosis of ovarian cancer: a systematic review. BJOG. 2005;112(7):857-865.
3. Goff BA, Mandel L, Muntz HG, Melancon CH. Ovarian carcinoma diagnosis. Cancer. 2000;89(10):2068-2075.
4. Zheng J, Benedict WF, Xu HJ, et al. Genetic disparity between morphologically benign cysts contiguous to ovarian carcinomas and solitary cystadenomas. J Natl Cancer Inst. 1995;87(15):1146-1153.
5. Marchbanks PA, Wilson H, Bastos E, et al. Cigarette smoking and epithelial ovarian cancer by histologic type. Obstet Gynecol. 2000;95(2):255-260.
6. Desaia PJ, Creasman WT. Clinical Gynecologic Oncology. 6th ed. St Louis: Mosby; 2002.
Middle-Aged Woman With Bilateral Staghorn Calculi
Chi-Fai NG, MBChB, Alexander C. Leung, MBBS, and Lane M. Robson, MD
A 48-year-old woman sought medical attention after an episode of gross hematuria associated with mild right-sided loin discomfort. She did not have urinary frequency, urgency, or dysuria. Her history included 3 urinary tract infections (UTIs); a Proteus species was cultured on each occasion. The family history was unremarkable. Other than mild loin tenderness, physical findings were normal.
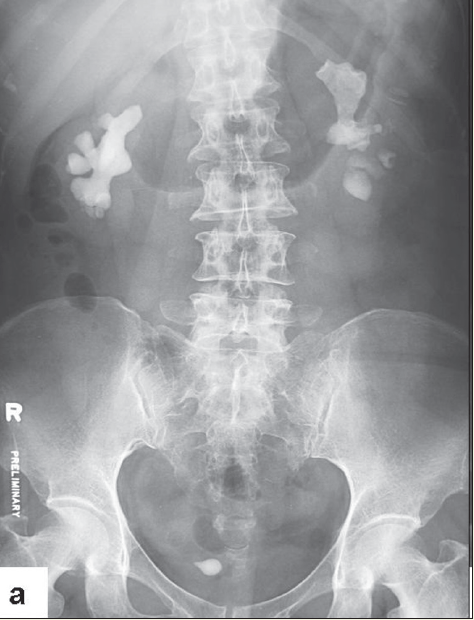
Laboratory testing. Urinalysis showed 5 to 10 white blood cells and 3 to 5 red blood cells per high-power field. Urine culture was negative. Plain radiography with a kidney-ureter-bladder (KUB) view revealed multiple opacities in the region of both kidneys and specifically in a location that corresponded to each renal pelvis. A subsequent intravenous urogram (IVU) confirmed the presence of bilateral renal staghorn calculi and a right ureteral stone within a ureterocele. A radioisotopic study showed the differential function of the right and left kidneys to be 44% and 56%, respectively, with scarring in the upper pole of the right kidney. Serum calcium, phosphate, urate, and blood urea (nitrogen, creatinine, and electrolyte levels) were normal.
The patient underwent transurethral incision of the right ureterocele and ureteroscopic removal of the ureteral stone. Simultaneous right percutaneous nephrolithotomy (PCNL) was performed, and a ureteral stent was inserted at the end of the procedure. Secondstage right PCNL for the residual stones was performed 2 weeks later, and all the stones were cleared. Left PCNL was also performed with clearance of all the residual stones. Stone analysis revealed that the calculi were composed of 76% magnesium ammonium phosphate (struvite) and 24% calcium carbonate (apatite).
Urolithiasis affects about 10% to 12% of the population worldwide, and the incidence is increasing.1,2 Without preventative intervention, up to 50% of patients have a recurrence within 5 years after successful treatment. Males and those with a family history of renal stones are more likely to be affected. Staghorn stones are slightly more common in females.3
Clinical manifestations. Renal stones are often asymptomatic. In contrast to ureteral stones, renal stones seldom present as an emergency. Typical symptoms of acute renal colic are intermittent colicky flank pain that might radiate to the lower abdomen or groin.4 Nausea and vomiting may be present.
The physical examination findings are either unremarkable or reveal mild tenderness with palpation of the affected kidney. Patients who have renal stones complicated by pyelonephritis are often febrile and toxic-looking and have tachycardia. In this setting, the tenderness with palpation of the affected kidney is usually considerable.
A large right upper caliceal renal stone is shown on a pretreatment radiograph. After one session of extracorporeal shockwave lithotripsy, stone fragments are scattered inside the mid and lower calices and steinstrasse formation is evident in the right lower ureter.
Diagnostic studies. Urinalysis typically shows hematuria, which is present in 85% to 90% of patients with a renal stone and is usually microscopic. White blood cells and bacteria suggest concomitant infection. Struvite crystals are usually coffin lid-shaped. Cystine crystals are hexagonal. Uric acid crystals are rhomboid, biconvex, or barrel-shaped. Calcium oxalate crystals can be bipyramidal, ovoid, biconcave, or dumbbell-shaped; they are birefringent, and appear as bright specks with polarized microscopy.
Urine pH can provide clues about the possible composition of the stone. If the urine pH is >7.5, the stone is probably infective in origin. If the urine pH is <5.5, a uric acid stone is more likely. Urine culture is important to rule out a coexisting UTI.5
Blood tests for urea, creatinine, electrolytes, calcium, and urate should be performed. If the patient has hypercalcemia, consider hyperparathyroidism. A 24-hour urine collection for calcium, phosphorus, uric acid, oxalate, cystine, citrate, sodium, magnesium, and creatinine should be ordered.
Plain radiography of the abdomen with a KUB view reveals up to 70% of renal stones. Ultrasonography or unenhanced helical CT can detect more than 90% of renal stones.6,7 IVU was formerly the study of choice to confirm the presence of the stone, to provide an anatomical outline of the urinary tract, and to identify the presence and the degree of obstruction. CT is commonly available and is now considered the study of choice.
A supplementary IVU is indicated for renal pelvic stones, for caliceal stones larger than 1 cm, and after failure of extracorporeal shockwave lithotripsy (ESWL).
For patients with large renal stones, such as staghorn calculi, or with a poorly functioning kidney, radioisotopic renography should be performed to assess the differential renal function.
Discussion. Staghorn calculi are branched stones that occupy a major part of the renal collecting system.8 These stones usually fill the renal pelvis and branch into several or all of the calices. Most staghorn stones are composed of mixtures of magnesium ammonium phosphate and calcium carbonate apatite, but cystine and uric acid stones can also present in this fashion.3
Staghorn stones composed of struvite are usually associated with UTI caused by a urea-splitting organism, the most common of which is Proteus mirabilis. Other urea-splitting bacteria include some Klebsiella and Pseudomonas species, Staphylococcus saprophyticus, and Ureaplasma urealyticum. The resultant alkaline urinary environment and the high urinary concentrations of ammonia, trivalent phosphate, and magnesium promote crystallization of magnesium ammonium phosphate, which leads to the formation of large, branched stones.8 Magnesium ammonium phosphate stones can form on a idus of a calcium oxalate renal stone.
Treatment. Untreated staghorn calculi are associated with eventual renal destruction and significant morbidity and mortality.9 Active treatment should be offered to patients with these stones.
Since its introduction in 1980, ESWL has become a common first-line treatment option for urinary stones, especially those <1 cm. The success rate is lower for large renal stones. There is a higher risk of obstruction because of the production of a large amount of small stone fragments or steinstrasse (stone street). For stones >2 cm, PCNL is a better option.
According to the American Urological Association (AUA) Nephrolithiasis Clinical Guidelines Panel on staghorn calculi, ESWL monotherapy is not recommended as a first-line treatment for staghorn stones, especially cystine stones. Rather, this therapy should be used only in combination with PCNL.8 A single staghorn stone of less than 4 cm that is heterogeneous and has a density similar to or less than that of the bone, and that is present in a normal collecting system, has the best response to ESWL.10,11 Contraindications to ESWL include pregnancy, uncontrolled bleeding tendency, severe skeletal deformity, morbid obesity, untreated UTI, aortic aneurysm, and renal artery aneurysm.12
A complicated staghorn stone is shown on a pretreatment radiograph and after removal by open surgery.
PCNL involves the creation of an access tract into the renal collecting system through which nephroscopy can be performed.4 PCNL is highly effective13; treatment outcomes are relatively independent of stone size and are uniformly high for stones in all locations.
The AUA recommends PCNL as the treatment of choice for most patients with a staghorn stone.8 For patients with extremely large or complex staghorn stones, combination therapy with ESWL might be necessary. PCNL has a stone-free rate close to that of open surgery.12 PCNL also has the advantages of lower morbidity, shorter operative time, shorter hospital stay, and earlier return to work.12
The use of flexible ureteroscopy and the wide availability of the holmium: YAG laser, which can fragment nearly all stone types to dust-like particles, allow the performance of retrograde intrarenal surgery for renal stones. Complications are relatively uncommon with modern ureteroscopy.14 The stone-free rate for a small to moderate-size stone is comparable to that of PCNL. The procedure is particularly useful in patients with renal anomalies such as horseshoe kidney and caliceal diverticulum. In these patients, the stone-free rate with ESWL is typically low because of poor clearance of stone fragments. Ureteroscopy is also an attractive option for patients in whom ESWL and PCNL are less effective or contraindicated, such as those who are pregnant or morbidly obese or who have a coagulopathy.8
Open surgery for renal calculi has now been supplanted by less invasive procedures.4 Studies have confirmed the advantages of endoscopic surgery (PCNL) over open surgery for staghorn stones.15,16 Open surgery is mainly reserved for patients with large, extensively branched, complex staghorn stones, those with altered renal anatomy, and those with coexisting renal abnormalities that require a simultaneous reconstructive open procedure. However, for a kidney with poor renal function (differential kidney function of less than 15%), simple nephrectomy might be more definitive and beneficial for the patient than multiple complicated endoscopic stone removal procedures.
After successful stone clearance, prophylactic measures are necessary to prevent stone recurrence. The composition of the stone should guide prophylactic therapy. For patients with struvite stones, predisposing factors for UTI, such as voiding dysfunction, vesicoureteral reflux, obstruction, and neurogenic bladder, should be identified and treated. Periodic urine cultures are needed to detect UTI.
For patients with a uric acid stone, a low-purine diet is advisable; medical treatment is indicated if hyperuricemia cannot be controlled by dietary modification. Increased fluid intake and alkalinization therapy should also be recommended to decrease the risk of uric acid crystal formation in the urine.
Patients with calcium-related stones should avoid foods with a high content of oxalate, such as wheat bran, spinach, cocoa, and nuts.17 The present consensus is that excessive dietary restriction of calcium intake is not recommended.17,18 Consumption of citrus fruit can help increase levels of urinary citrate, which forms a complex with calcium and minimizes the risk of calcium calculi formation.19 Excessive salt intake should be avoided because a high sodium load in the renal tubules will result in increased excretion of calcium into the tubular fluid.20
References:
1. Lotan Y, Cadeddu JA, Pearle MS. International comparison of cost effectiveness of medical management strategies for nephrolithiasis. Urol Res. 2005;
33(3):223-230.
2. Robertson WG. Is prevention of stone recurrence financially worthwhile? Urol Res. 2006;34(2):157-161.
3. Akagashi K, Tanda H, Kato S, et al. Characteristics of patients with staghorn calculi in our experience. Int J Urol. 2004;11(5):276-281.
4. Miller NL, Lingeman JE. Management of kidney stones. BMJ. 2007;334:468-472.
5. Leung AK, Robson WL. Urinary tract infection in infancy and childhood. Adv Pediatr. 1991;38:257-285.
6. Smith RC, Verga M, McCarthy S, et al. Diagnosis of acute flank pain: value of unenhanced helical CT. AJR. 1996;166(1):97-101.
7. Niall O, Russell J, MacGregor R, et al. A comparison of noncontrast computerized tomography with excretory urography in the assessment of acute flank pain. J Urol. 1999;161(2):534-537.
8. Preminger GM, Assimos DG, Lingeman JE, et al. Chapter 1: AUA guideline on management of staghorn calculi: diagnosis and treatment recommendations. J Urol. 2005;173(6):1991-2000.
9. Blandy JP, Singh M. The case for a more aggressive approach to staghorn stones. J Urol. 1976;115:505-506.
10. Murshidi MS. Simple radiological indicators for staghorn calculi response to ESWL. Int Urol Nephrol. 2006;38(1):69-73.
11. El-Assmy A, El-Nahas A, Madbouly K. Extracorporeal shock-wave lithotripsy monotherapy of partial staghorn calculi: prognostic factors and longterm clinical results. Scand J Urol Nephrol. 2006;40(4):320-325.
12. Krambeck AE, Gettman MT, Rohlinger AL, et al. Diabetes mellitus and hypertension associated with shock wave lithotripsy of renal and proximal ureteral stones at 19 years of followup. J Urol. 2006;175(5):1742-1747.
13. Pearle MS, Lingeman JE, Leveillee R, et al. Prospective, randomized trial comparing shock wave lithotripsy and ureteroscopy for lower pole caliceal calculi 1 cm or less. J Urol. 2005;173(6):2005-2009.
14. Knoll T, Alken P, Michel MS. Progress in management of ureteric stones. EAU Update Series. 2005;3:44-50.
15. Al-Kohlany KM, Shokeir AA, Mosbah A, et al. Treatment of complete staghorn stones: a prospective randomized comparison of open surgery versus percutaneous nephrolithotomy. J Urol. 2005;173(2):469-473.
16. Brannen GE, Bush WH, Correa RJ, et al. Kidney stone removal: percutaneous versus surgical lithotomy. J Urol. 1985;133(1):6-12.
17. Tiselius HG, Ackermann D, Alken P, et al. Guidelines on urolithiasis. Eur Urol. 2001;40(4):362-371.
18. Teichman JM. Acute renal colic from ureteral calculus. N Engl J Med. 2004;350(7):684-693.
19. Micali S, Grande M, Sighinolfi MC, et al. Medical therapy of urolithiasis. J Endourol. 2006;20(11):841-847.
20. Westenberg A, Harper M, Zafirakis H, et al. Bladder and renal stones: management and treatment. Hosp Med. 2002;63(1):34-41.
Emphysematous Cystitis
Alexander SY, MD, and Shobhana Chaudhari, MD
A 77-year-old woman with hypertension, diabetes mellitus with neuropathy and nephropathy, coronary artery disease, and previous stroke with residual right hemiparesis was hospitalized after a sudden onset of abdominal pain, nausea, and vomiting. She also reported subjective fever, dysuria, and foul-smelling urine.
Physical examination. The patient was afebrile, her blood pressure was 170/90 mm Hg, and her heart rate was 104 beats per minute. The hypogastric region was tender with no rebound. Other physical findings were normal.
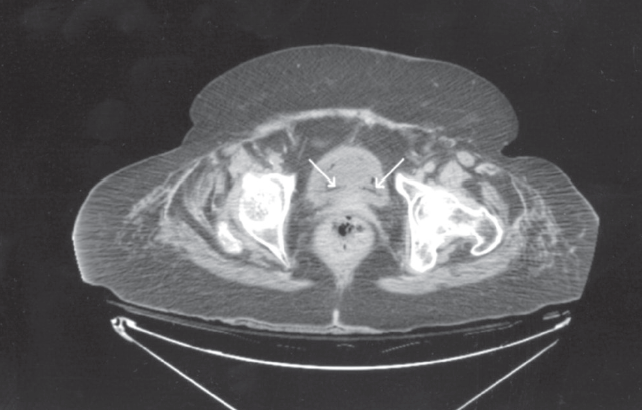
Laboratory testing. White blood cell count was 9820/µL, blood glucose level was 286 mg/dL, and her glycosylated hemoglobin was 7.1%. Urinalysis findings were consistent with urinary tract infection (UTI). A CT scan of the abdomen revealed air within the wall of the urinary bladder, compatible with emphysematous cystitis. Because of the patient’s age and comorbidities, she was empirically treated with piperacillin/tazobactam. Blood cultures were negative. Urine culture later grew Escherichia coli.
Discussion. Emphysematous cystitis is a commonly missed, relatively unknown disease. Although the pathogenesis of the gas formation is still unclear, metabolism of glucose and albumin in the urine by gas-forming organisms and impaired host response with poor vascular perfusion are 2 postulated theories.1-4 E coli and pneumoniae are commonly isolated; however, other organisms, such as Clostridium, Pseudomonas, Proteus, Enterococcus, Aspergillus, and Candida, have been reported.2 Risk factors include female gender, diabetes mellitus, age older than 60 years, debilitated states, neurogenic bladder, recurrent UTI, urinary stasis secondary to bladder outlet obstruction, alcoholism, and malnutrition.1
When intraluminal gas is present, other entities, such as a recent urinary tract instrumentation, trauma, and vesicocolic/vesicovaginal fistulas, should also be considered.2,4,5 Clinical presentations range from no symptoms, descriptive pneumaturia, and irritative voiding symptoms to acute abdomen and severe sepsis.2,3 Thus, a high index of suspicion for emphysematous cystitis is required. The condition is usually diagnosed incidentally by plain abdominal film, ultrasonography, or CT scan findings. Other modalities include direct visualization during cystoscopy or laparotomy and biopsy. 2,3
However, CT remains the preferred diagnostic method, because of its high sensitivity and specificity in detecting gas and the extent and severity of disease and in differentiating other causes of intraluminal gas formation.1,2,5
References:
1. Leclercq P, Hanssen M, Borgoens P, et al. Emphysematous cystitis. CMAJ. 2008;178(7):836.
2. Thomas AA, Lane BR, Thomas AZ, et al. Emphysematous cystitis: a review of 135 cases. BJU Int. 2007;100(1):17-20.
3. Chong SJ, Lim KB, Tan YM, et al. Atypical presentations of emphysematous cystitis. Surgeon. 20053:109-112.
4. Choong KK. Sonographic detection of emphysematous cystitis. J Ultrasound Med. 2003;22(2):847-849.
5. Bobba RK, Arsura EL, Sarna PS, Sawh AK. Emphysematous cystitis: an unusual disease of the Genito-Urinary system suspected on imaging. Ann Clin Microbiol Antimicrob. 2004;3:20.