
A Collection of Kidney-Related Issues
Elevated Hematocrit in Man Receiving Hemodialysis
Crystal Denlinger, MD, and Ronald N. Rubin, MD
A 50-year-old man with end-stage renal disease secondary to long-standing hypertension had an elevated hematocrit and progressively increasing hemoglobin levels. For the past 7 years, he had been receiving hemodialysis 3 times a week. He denied headache, flushing, easy bruising, bleeding, nausea, vomiting, chest pain, dyspnea, and other symptoms. He was not receiving exogenous erythropoietin.
 History. The patient had a positive result on a tuberculin skin test about 10 years earlier and received appropriate prophylaxis. He had undergone arteriovenous (AV) fistula placement in 1999 and back surgery and an appendectomy in the 1980s. His medications included hydralazine, 75 mg every 6 hours; amlodipine, 10 mg qd; calcium carbonate, 1000 tid; and metoprolol, 50 mg bid. He had no drug allergies; however, aspirin and warfarin had caused upper GI bleeding. His mother and sister both died of breast cancer, but he had no family history of kidney disease or blood dyscrasia. He had smoked 1 pack of cigarettes a day for 35 years; he denied use of alcohol or illicit drugs.
History. The patient had a positive result on a tuberculin skin test about 10 years earlier and received appropriate prophylaxis. He had undergone arteriovenous (AV) fistula placement in 1999 and back surgery and an appendectomy in the 1980s. His medications included hydralazine, 75 mg every 6 hours; amlodipine, 10 mg qd; calcium carbonate, 1000 tid; and metoprolol, 50 mg bid. He had no drug allergies; however, aspirin and warfarin had caused upper GI bleeding. His mother and sister both died of breast cancer, but he had no family history of kidney disease or blood dyscrasia. He had smoked 1 pack of cigarettes a day for 35 years; he denied use of alcohol or illicit drugs.
Physical examination. The patient weighed 107.4 kg (263.3 lb). Heart rate was 97 beats per minute; blood pressure, 85/64 mm Hg; and oxygen saturation, 96% on room air. Pupils were reactive bilaterally with pink conjunctiva. Mucous membranes were moist. There was no jugular venous distention, and his heartbeat was regular, with no murmurs. Lungs were clear. Abdomen was soft and nontender. No abdominal or flank masses were found. An AV fistula was noted in the left upper extremity; there was no edema in the lower extremities.
Laboratory testing. White blood cell count was 8300/µL; hemoglobin level, 16.5 g/dL with hematocrit, 48.6%; and platelet count, 202,000/µL. Results of a chemistry panel included the following levels: blood urea nitrogen, 45 mg/dL; creatinine, 10.3 mg/dL; calcium, 7.7 mg/dL; albumin, 4.6 g/dL; total protein, 9.9 g/dL; alkaline phosphatase, 393 U/L; alanine aminotransferase, 16 U/L; and aspartate aminotransferase, 66 U/L.
Plasma erythropoietin level was elevated at 40.5 mU/mL. Reticulocyte count was 2.5%, with an iron level of 47 µg/dL, a total iron-binding capacity of 275 µg/dL, and a saturation iron binding capacity of 17%.
Carboxyhemoglobin level was 3.5%. Results of pulmonary function tests were otherwise normal.
A report of an MRI scan of the patient's abdomen performed in 2002 described numerous hemorrhagic and nonhemorrhagic renal cysts bilaterally. The largest of these, on the right kidney, measured 3.5 cm in diameter.
A recent MRI scan of the abdomen showed numerous well-defined intraparenchymal and exophytic cysts scattered diffusely throughout both kidneys (Figures 1 and 2). The largest, in the mid-pole of the anterior right kidney, measured 2.9 x 2.8 x 2.9 cm. Compared with the 2002 study, the number of cystic lesions had increased markedly; very little renal parenchyma was visible. Some of these cysts were hemorrhagic; none showed abnormal enhancement.
Erythrocytosis, or polycythemia, is characterized by an elevated red blood cell mass. It may result from increased proliferation of erythrocyte progenitors or from abnormal erythrocyte regulation. Clinically, it usually manifests as hemoglobin levels above 17.7 g/dL in men or 15.7 g/dL in women and a hematocrit greater than 51% in men or 48% in women. Symptoms of the hyperviscosity characteristic of erythrocytosis may include headache, dizziness, light-headedness, a congested sensation, and worsening of exercise tolerance.1 Include in the workup determination of serum erythropoietin level, measurement of red cell mass and plasma volume, and determination of oxygen saturation.2
Discussion. This is the most common cause of secondary polycythemia. Smoking-related erythrocytosis results from a carboxyhemoglobin-induced increase in red blood cell mass with a concurrent decrease in plasma volume. The carbon monoxide that enters the bloodstream when cigarette smoke is inhaled binds to heme iron with an affinity 200 times greater than that of oxygen and forms carboxyhemoglobin. As carboxyhemoglobin levels increase, the functional hemoglobin in the blood is reduced proportionally and oxygen delivery to tissues is impaired.3 Carboxyhemoglobin levels of greater than 4% can cause erythrocytosis.1
Treatment of polycythemia caused by cystic kidney disease may include drainage or resection of large cysts, removal of renal tumors, or nephrectomy of native kidneys at the time of transplantation. Phlebotomy with hemodialysis to maintain a hematocrit under 48% in men or 45% in women may also be effective. However, because phlebotomy may deplete existing iron stores, iron supplementation is necessary.4,5
Because this patient's polycythemia was borderline and he had no symptoms, phlebotomy was not mandatory. However, he did undergo intermittent phlebotomy during dialysis as a precautionary measure. When he returned 1 month later for follow-up, his hemoglobin level was 14.9 g/dL. He was counseled to stop smoking and remains on the kidney transplant list.
References:
1. Golde DW, Hocking WG, Koeffler HP, Adamson JW. Polycythemia: mechanisms and management. Ann Intern Med.1981;95(1):71-87.
2. Tefferi A, Spivak JL. Polycythemia vera: scientific advances and current practice. Semin Hematol. 2005;42(4):206-220.
3. Smith JR, Landaw SA. Smokers' polycythemia. N Engl J Med. 1978;298(1):6-10.
4. Hoffman R, Baker KR, et al. The polycythemias. In: Hoffman R, Benz EJ, Shattil SJ, et al, eds. Hematology: Basic Principles and Practice. 4th ed. New York, NY: Churchill Livingstone; 2004.
5. Hadimeri H, Norden G, Friman S, Nyberg G. Autosomal dominant polycystic kidney disease in a kidney transplant population. Nephrol Dial Transplant. 1997;12(7):1431-1436.
Acute Glomerulonephritis in a Young Woman
Lisa Wray, MD, and Anthony Donato, MD
A 26-year-old woman presented with a 1-week history of pleuritic chest pain and abdominal pain, which was associated with nausea but unrelated to food intake or bowel movements. She had also had gross hematuria for the past 10 days and swelling around her eyes and ankles as well as fatigue and arthralgias for 2 weeks.
She reported having "the flu" a month earlier. She denied injection drug use, cough, and sinus complaints. Her 3 young children had an upper respiratory tract illness at about the same time as her flu-like symptoms last month. She took no long-term medications.
Physical examination. The patient appeared tired but was in no acute distress. Temperature was 36.9ºC (98.4ºF); heart rate, 60 beats per minute; respiration rate, 20 breaths per minute; blood pressure, 132/76 mm Hg; and oxygen saturation measured by pulse oximetry was 100% while breathing ambient air. Mild periorbital edema was noted. Chest pain was reproducible by palpation and by deep inspiration. Bowel sounds were present. Abdomen was diffusely tender without rebound tenderness or guarding. There was edema of the lower extremities to mid-tibia. Arthralgias without arthritis were noted in the hands.
 Laboratory testing. Complete blood cell count revealed normocytic, normochromic anemia and thrombocytosis. Other laboratory values included an erythrocyte sedimentation rate of 142 mm/h; blood urea nitrogen, 31 mg/dL; serum creatinine, 1.3 mg/dL (baseline level was unknown); and serum albumin, 1.9 g/dL. Blood cultures were negative. Urinalysis showed a large amount of blood, 100 mg/dL of protein, and 10 to 12 white blood cells and 35 to 40 red blood cells per high-power field. C3 complement level was 6 mg/dL (normal, 59-120 mg/dL). Chest radiographic findings were normal.
Laboratory testing. Complete blood cell count revealed normocytic, normochromic anemia and thrombocytosis. Other laboratory values included an erythrocyte sedimentation rate of 142 mm/h; blood urea nitrogen, 31 mg/dL; serum creatinine, 1.3 mg/dL (baseline level was unknown); and serum albumin, 1.9 g/dL. Blood cultures were negative. Urinalysis showed a large amount of blood, 100 mg/dL of protein, and 10 to 12 white blood cells and 35 to 40 red blood cells per high-power field. C3 complement level was 6 mg/dL (normal, 59-120 mg/dL). Chest radiographic findings were normal.
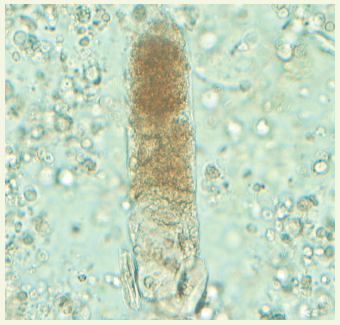
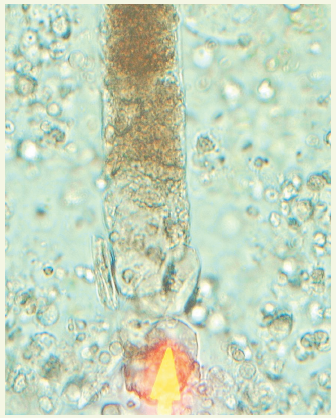
Results of a urinary sediment examination revealed red blood cell casts—a pathognomonic finding for acute glomerulonephritis (Figure). The antistreptolysin O (ASO) titer was 1590 u/mL (normal, 0-117 u/mL).
Glomerular hematuria may herald acute renal failure. This patient's urinary sediment with red cell casts as well as her proteinuria, edema, and hypocomplementemia were all signs of nephritis and prompted further evaluation.
The differential diagnosis of acute glomerulonephritis includes conditions that are associated with low complement levels (post-streptococcal glomerulonephritis, endocarditis, lupus nephritis, and cryoglobulinemia) and those that are not (Henoch-Schönlein purpura, IgA nephropathy, Goodpasture syndrome, and Wegener granulomatosis). This patient's elevated ASO titer (present in 50% to 70% of cases),1 active urinary sediment, and hypocomplementemia confirmed the diagnosis of poststreptococcal glomerulonephritis.
 Discussion. Typically a disease of children, poststreptococcal glomerulonephritis is caused by antibodies to unknown antigens of type 12 group A β-hemolytic streptococci. Symptoms develop 1 to 4 weeks after streptococcal infection of the pharynx or skin. Hematuria associated with poststreptococcal glomerulonephritis should be distinguished from hematuria that develops within 1 day of upper respiratory tract symptoms in patients with IgA nephropathy; in the latter setting, hematuria frequently recurs.
Discussion. Typically a disease of children, poststreptococcal glomerulonephritis is caused by antibodies to unknown antigens of type 12 group A β-hemolytic streptococci. Symptoms develop 1 to 4 weeks after streptococcal infection of the pharynx or skin. Hematuria associated with poststreptococcal glomerulonephritis should be distinguished from hematuria that develops within 1 day of upper respiratory tract symptoms in patients with IgA nephropathy; in the latter setting, hematuria frequently recurs.
Poststreptococcal glomerulonephritis is typically self-limited. Ninety-five percent of children recover spontaneously. Progression to chronic renal failure occurs in up to 20% of adults.2 In adults who recover spontaneously, the elevated creatinine level returns to baseline within 4 weeks and complement levels normalize within 8 weeks. Hematuria usually resolves within 6 months, whereas proteinuria may persist for 3 years.
Outcome of the case. In retrospect, the patient's flu-like illness 1 month earlier was probably her initial streptococcal infection. She was given amoxicillin for 14 days to eradicate any remaining infection. The arthralgias and chest pains resolved 2 days into therapy, and blood urea nitrogen and creatinine levels decreased to 16 and 0.9 mg/dL, respectively, by the time of discharge on day 3. Her blood pressure, hematuria, proteinuria, and serum creatinine and complement levels will be closely monitored for any indication of hypertension or renal damage.
References:
1. Berrios X, Lagomarsino E, Solar E, et al. Post-streptococcal acute glomerulonephritis in Chile—20 years of experience. Pediatr Nephrol. 2004;19(3):306-312.
2. Pinto SW, Sesso R, Vasconcelos E, et al. Follow-up of patients with epidemic poststreptococcal glomerulonephritis. Am J Kidney Dis. 2001;38(2):248-255.
Raccoon Eyes
Diego Maselli, MD, and Stephen Richey, MD, MPH
A 58-year-old man with type 2 diabetes, nephrolithiasis, and benign prostatic hyperplasia presented with bilateral periorbital ecchymoses and left subconjunctival hemorrhage. The ecchymoses had spontaneously appeared 3 days earlier; the patient had no history of trauma or falls. He also had difficulty in voiding, characterized by increased frequency, hesitancy, and diminished urine stream. The urinary symptoms had been progressively worsening for a week and were now accompanied by severe intermittent abdominal pain.

Physical examination. The patient had no petechiae and no other ecchymoses or signs of hemorrhage. Palpation elicited mild tenderness in all abdominal quadrants; the pain was worse in the suprapubic region. There was no fullness or palpable masses. The rectal examination revealed a markedly enlarged, nontender prostate.
The patient was asked to urinate under observation. During micturition, he strained with tremendous effort, which caused marked facial plethora and diaphoresis. He then stated that he routinely strained for 6 to 7 minutes, with only minimal urine production. Placement of a Foley catheter relieved 1.2 L of urine. His abdominal pain immediately resolved.
Laboratory results showed a blood urea nitrogen level of 98 mg/dL, serum creatinine level of 11.9 mg/dL, normal complete blood cell count and coagulation studies, and a prostatic-specific antigen level of 134 ng/mL. A renal ultrasonogram revealed hydronephrosis with nephrolithiasis in multiple calices bilaterally.
The periorbital ecchymosis slowly faded over the next few days. The creatinine level at discharge was 1.3 mg/dL. An outpatient prostate biopsy revealed adenocarcinoma.

Discussion. “Raccoon eyes” or bilateral periorbital ecchymoses can result from direct trauma to the eye and surrounding soft tissues,1 basal skull fracture,2 rhinoplasty,3 amyloidosis, 4,5 malignancy,6-8 trigeminal autonomic cephalgia,9 and vigorous sneezing10 or coughing.11 This patient’s periorbital ecchymoses were most likely caused by the increased pressure in the capillary beds surrounding the palpebral region that occurred during straining. This Valsalva maneuver–like mechanism is similar to that of prolonged sneezing or coughing.
Although the combination of renal failure and periorbital purpura aroused suspicion of amyloidosis initially, a renal biopsy or fat pad biopsy was deferred because the creatinine level normalized after the outflow obstruction was relieved and no other clinical manifestations of systemic amyloidosis were observed. Platelet dysfunction secondary to uremia was a possible risk factor for bleeding in this patient; however, this disorder is more common in those with chronic renal failure.12,13
References:
1. Ghazi-Nouri SM, Vote BJ, Sullivan PM. Periorbital ecchymosis as a sign of perforating injury of the globe. Clin Experiment Ophthalmol. 2005;33(2):194-196.
2. Odebode TO, Ademola-Popoola DS, Ojo TA, Ayanniyi AA. Ocular and visual complications of head injury. Eye (Lond). 2005;19(5):561-566.
3. Li Y, Xu G. Complications of nasal endoscopic surgery [in Chinese]. Zhonghua Er Bi Yan Hou Ke Za Zhi.1998;33(3):142-145.
4. Bernardini FP. Periocular and orbital amyloidosis. Ophthalmology. 2007;114(6):1232.
5. Berge E, Bernard JL, Dryll A. Value of periorbital ecchymosis in the diagnosis of amyloidosis [in French]. Presse Med. 1991;20(14):658.
6. Dober I, Stranzinger E, Kellenberger CJ, Huisman TA. Periorbital ecchymosis— trauma or tumor? [in German]. Praxis (Bern 1994). 2007;96(2):811-814.
7. Ahmed S, Goel S, Khandwala M, et al. Neuroblastoma with orbital metastasis: ophthalmic presentation and role of ophthalmologists. Eye(Lond). 2006;20(4):466-470.
8. Schwartz RA, Spicer MS, Thomas I, et al. Ecchymotic Kaposi’s sarcoma. Cutis. 1995;56(2):104-106.
9. Attanasio A, D’Amico D, Frediani F, et al. Trigeminal autonomic cephalgia with periorbital ecchymosis, ocular hemorrhage, hypertension and behavioral alterations. Pain. 2000;88(1):109-112.
10. Maramattom BV. Raccoon eyes following vigorous sneezing. Neurocrit Care. 2006;4(2):151-152.
11. Chuang YY, Chiu CH, Wong KS, et al. Severe adenovirus infection in children. J Microbiol Immunol Infect. 2003;36(1):37-40.
12. Hassan AA, Kroll MH. Acquired disorders of platelet function. Hematology Am Soc Hematol Educ Program. 2005:403-408.
13. Escolar G, Díaz-Ricart M, Cases A. Uremic platelet dysfunction: past and present. Curr Hematol Rep. 2005;4(5):359-367.
Triamterene Kidney Stones
Fasdi I. Jabr, MD and Nedaa Skeik, MD
 A 64-year-old woman with a history of recurrent kidney stones presented with severe left flank pain radiating to the left lower quadrant of 4 days’ duration. She brought with her a large fragmented 70-mg stone that she had passed in urine. Her medications included hydrochlorothiazide, 25 mg/triamterene, 37.5 mg.
A 64-year-old woman with a history of recurrent kidney stones presented with severe left flank pain radiating to the left lower quadrant of 4 days’ duration. She brought with her a large fragmented 70-mg stone that she had passed in urine. Her medications included hydrochlorothiazide, 25 mg/triamterene, 37.5 mg.
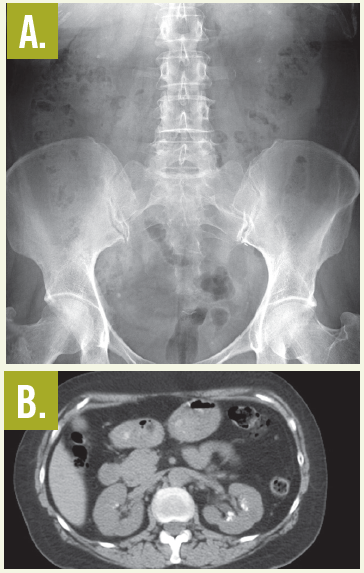
Laboratory testing. An abdominal radiograph (A) and a CT scan of the kidneys, ureters, and bladder (B) showed bilateral renal calcifications. On the right, the largest was 3 mm, and on the left, multiple punctate calcifications were evident. Urinalysis was positive for trace blood and trace leukocytes. The analysis of the stone revealed triamterene composition. The patient underwent successful placement of ureteral stents to help passage of the stones followed by lithotripsy.
Discussion. In the 1970s, triamterene was the major cause of drug-induced renal calculi.1 In a 1980 study, the estimated annual incidence of triamterene lithiasis was 1 per 1500 users of triamterene/hydrochlorothiazide.2 Triamterene was found in 0.4% (181 of 50,000) of renal calculi submitted for analysis.2 This percentage has probably changed in recent years because indinavir and sulfadiazine are now the most common causes of drug-containing renal stones.1,3 Triamterene is still responsible, however, for many drug-induced calculi.
Both unchanged triamterene and its metabolites, hydroxytriamterene and sulfate ester of hydroxytriamterene, are present in triamterene stones.4 Up to one-third of triameterene stones consist entirely of triamterene.2,5 In the remainder, triameterene formed the nucleus of the stone or was deposited with calcium oxalate or uric acid; this finding suggests that in the majority of cases, triamterene lithiasis develops in persons who have had renal stones.2 It becomes incorporated into existing stone nidi by binding to the protein matrix found in all kidney stones.6
Treatment. The treatment consists of discontinuation of medication and lithotripsy, because the calculi cannot be dissolved by pH manipulation.3 On plain radiographs, triamterene stones are—as in this case—faintly radiopaque and are less dense than calcium oxalate stones. They are more detectable on a CT scan of the kidneys, ureters, and bladder.
This case illustrates the need to be cautious in the use of triamterene, particularly in patients who are predisposed to nephrolithiasis or who have a prior history of kidney stones, to avoid the formation of new calculi. This caution applies even when triamterene is used in combination with hydrochlorothiazide.2
References:
1. Daudon M, Jungers P. Drug-induced renal calculi: epidemiology, prevention and management. Drugs. 2004;64(3):245-275.
2. Ettinger B, Oldroyd NO, Sorgel F. Triamterene nephrolithiasis. JAMA.1980;244(21):2443-2445.
3. Matlaga BR, Shah OD, Assimos DG. Drug-induced urinary calculi. Rev Urol. 2003;5(4):227-231.
4. Sorgel F, Ettinger B, Benet LZ. The true composition of kidney stones passed during triamtrene therapy. J Urol. 1985;134(5):871-873.
5. Carr MC, Prien EL Jr, Babayan RK. Triamterene nephrolithiasis: renewed attention is warranted. J Urol. 1990;144(6):1339-1340.
6. Werness PG, Bergert JH, Smith LH. Triamterene urolithiaisis: solubility, pk, effect on crystal formation, and matrix binding of triamterene and its metabolites. J Lab Clin Med. 1982;99(2):254-262.