
Progressive Dyspnea in a 65-Year-Old Woman
Churg-Strauss Syndrome Presenting as Refractory Asthma
A 65-year-old Caucasian female with a history of refractory asthma complains of progressive dyspnea, arthralgias, and bilateral lower extremity rash. Her asthma medications include albuterol, fluticasone/salmeterol, and recently initiated montelukast.
Physical examination. Physical examination was remarkable for bilateral expiratory wheezes with fine crackles and palpable purpura on the dorsal aspect of both feet.
________________________________________________________________________________________________________________________________________________
Related Content
Acute Dyspnea: Is the Cause Cardiac or Pulmonary—or Both?
Adjunct Therapies to Treat Dyspnea in Adult Patients with Moderate to Severe Asthma
________________________________________________________________________________________________________________________________________________
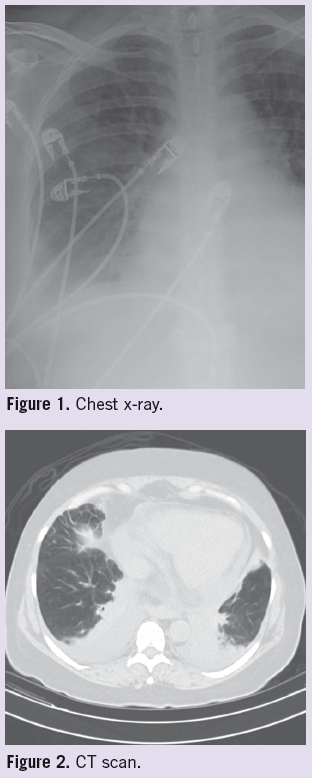 Laboratory tests. Initial laboratory workup revealed a leukocytosis with profound peripheral eosinophilia of 46.7%, as well as an elevated erythrocyte sedimentation rate, rheumatoid factor, and IgE. Antinuclear antibody, anti-neutrophil cytoplastmic antibody (ANCA), and cryoglobulins tests were negative. Chest x-ray showed bilateral pleural effusions and patchy infiltrates (Figure 1). Follow-up noncontrast chest CT confirmed bilateral patchy infiltrates (Figure 2).
Laboratory tests. Initial laboratory workup revealed a leukocytosis with profound peripheral eosinophilia of 46.7%, as well as an elevated erythrocyte sedimentation rate, rheumatoid factor, and IgE. Antinuclear antibody, anti-neutrophil cytoplastmic antibody (ANCA), and cryoglobulins tests were negative. Chest x-ray showed bilateral pleural effusions and patchy infiltrates (Figure 1). Follow-up noncontrast chest CT confirmed bilateral patchy infiltrates (Figure 2).
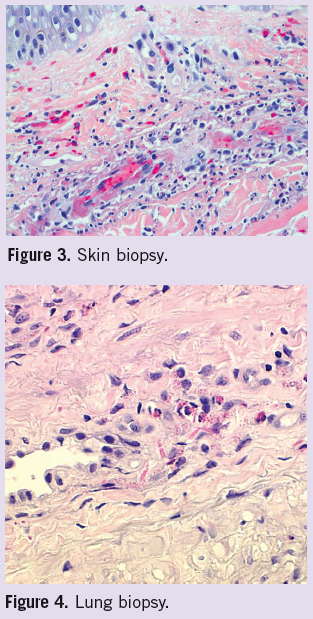
Diagnosis. Due to continued clinical deterioration, she was admitted to the hospital and initiated on empiric antibiotics and steroid therapy with marked improvement. Skin biopsy of her rash showed a leukocytoclastic vasculitis with prominent eosinophils (Figure 3). Bronchoscopy with subsequent transbronchial lung biopsy showed eosinophilic vasculitis and eosinophilic interstitial pneumonitis—classic for Churg-Strauss vasculitis (Figure 4).
Treatment. Montelukast was discontinued and prednisone was increased to 50 mg twice daily with continued improvement. The patient was discharged from the hospital with a slow prednisone taper and plans for steroid-sparing therapy as an outpatient. The patient responded very well to cyclophosphamide and eventually was taken off therapy without disease recurrence. She never restarted a leukotriene modifying agent (LTMA).
Discussion. Churg-Strauss syndrome (CSS) is a multisystem disorder characterized by eosinophilia, asthma, and necrotizing vasculitis, which affects small- to medium-sized arteries. Peripheral nerves, lung, and skin are most frequently involved, but any organ system can be affected by this disease with its wide range of clinical manifestations.1,2
Diagnosis can be made by meeting 4 of 6 established criteria: asthma, eosinophilia (>10% on differential), mono- or polyneuropathy, transient pulmonary opacities, paranasal sinus abnormalities, and extravascular eosinophilia on biopsy.2,3 Despite their absence in this case, ANCA are found in up to 60% of patients. The majority of these are against myeloperoxidase with a perinuclear staining pattern (MPO-ANCA or
P-ANCA).4
Early recognition is essential for appropriate treatment and the prevention of irreversible organ damage. Corticosteroids are the cornerstone of initial treatment of CSS, but additional immunosuppressive treatment (eg, azathioprine or cyclophosphamide) is required in cases of treatment failure or relapse.5 Remission rates with these therapies are reported in the literature as 81% to 91%, and chances of relapse increase with time. Factors found to portend a poor prognosis are proteinuria, elevated creatinine, GI involvement, cardiomyopathy, and neurologic involvement.4,6 An increasing number of case reports and review articles describe an association between LTMAs and CSS.3,7
 A systematic review discusses data from 62 cases of this kind, 2 cases of which CSS resolved with discontinuation of the LTMA alone.3 Another study shows a 4.5-fold increase in CSS with montelukast therapy, but offers that perhaps escalating asthma severity may be confounding.7
A systematic review discusses data from 62 cases of this kind, 2 cases of which CSS resolved with discontinuation of the LTMA alone.3 Another study shows a 4.5-fold increase in CSS with montelukast therapy, but offers that perhaps escalating asthma severity may be confounding.7
References:
1.Watts, RA, Lane SE, Bentham G, et al. Epidemiology of systemic vasculitis: a ten-year study in the United Kingdom, Arthritis Rheum. 2000;43:414-419.
2.Masi, AT, Hunder GG, Lie JT, et al. The American College of Rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (allergic granulomatosis and angitis). Arthritis Rheum. 1990;33:1094-1100.
3.Nathani N, Little MA, Kunst H, et al. Churg-Strauss syndrome and leukotriene antagonist use: a respiratory perspective. Thorax. 2008;63:883-888,
4.Mukhtyar C, Flossmann O, Hellmich B, et al. Outcomes from studies of antineutrophil cytoplasm antibody associated vasculitis: a systematic review by the European League Against Rheumatism systemic vasculitis task force. Ann Rheum Dis. 2008;67:1004-1010.
5.Pagnoux C, Guilpain L. Churg-Strauss syndrome. Curr Opin Rheumatol. 2007;19:25-32.
6.Guillevin L, Cohen P, Gayraud M, et al. Churg-Strauss syndrome. Clinical study and long-term follow-up of 96 patients. Medicine (Baltimore). 1999;78:26-37.
7.Hauser T, Mahr A, Metzler C, et al. The leukotriene receptor antagonist montelukast and the risk of Churg-Strauss syndrome: a case-crossover study. Thorax. 2008;63:677-682.