
A Chilling Case
A 65-year-old woman was brought to the emergency department (ED) by emergency medical service staff (EMS) after being found down and unresponsive in the snow. Heart and respiration rate were the only obtainable onsite vitals—heart rate in the 20s and respiratory rate of 8—and the attending EMS used bag valve mask (BVM) to provide assisted ventilations to the patient during transport to the hospital. Due to a medical command call placed by EMS prior to arrival, any further interventions (eg, intubation, atropine) were held at the recommendation of the medical command physician. On arrival to the ED, the patient had the following vital signs: heart rate, 36; respiratory rate, 10; peripheral capillary oxygen saturation, 93%; temperature, 22.9 C (rectal); and blood pressure, 76/41
PHYSICAL EXAMINATION
The patient was obtunded and cold to the touch. She was taking spontaneous breaths at a rate of 10/minute and was being assisted with BVM. She was noted to have groaning on exhalation. Her pupils were equal and sluggishly reactive to light and her head was without signs of trauma. She had palpable carotid pulses. Her lungs were clear bilaterally. She was noted to have abrasions to the bilateral shins, and her extremities were extremely cold to touch with no palpable peripheral pulses. Her abdomen was normal. The patent was opening her eyes spontaneously and was noted to have occasional spontaneous movement of all 4 extremities.
Two liters of warmed normal saline was infused and a Bair Hugger device was placed over her torso. A temperature sensing foley catheter was placed.
An EKG was obtained which is seen below. (Figure 1).
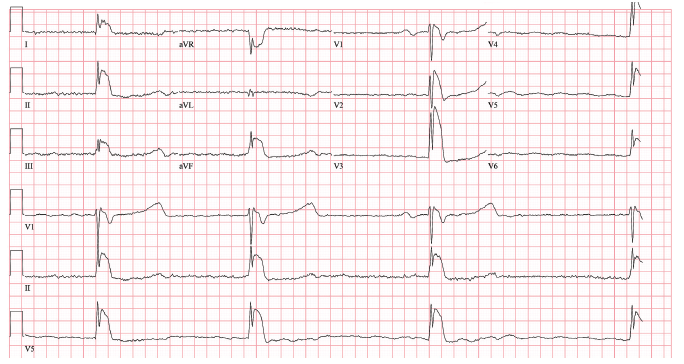
The patient continued to maintain oxygenation with bagging; therefore a decision was made to withhold intubation given the risk of precipitating an arrhythmia.
During rewarming in the ED, the patient was noted to have increased spontaneous movement of the extremities and increased moaning.
Labs demonstrated a mild leukocytosis with a mildly elevated lactate (2.2 mmol/L) and an arterial blood gas demonstrated a mixed respiratory and metabolic acidosis. The
following labs were unremarkable: liver function test, basic metabolic panel, thryrold stimulating hormone, lipase, magnesium, phosphate, urinalysis, urine tox, ethanol, salicylate, acetaminophen, and troponin.
What's Your Diagnosis?
A. Early repolarization (normal variant)
B. Osborn wave (J-wave) associated with hypothermia
C. Acute pericarditis
D. Myocardial infarction
(Answer and discussion on next page)
Answer: Osborn wave (J-wave) associated with hypothermia
DISCUSSION
This patient’s EKG demonstrated the classic Osborn wave (or J-wave) seen in approximately 80% of patients with a core temperature <35⁰C. The Osborn wave is thought to be secondary to slowed cardiac conduction and repolarization within the heart1, more specifically a slowing of the action potential notch in the epicardium but not in the endocardium2, although this theory has yet to be proven. As the core temperature drops below 32⁰C, the EKG may also demonstrate sinus bradycardia, prolonged PR interval, AV block, prolonged QT interval, junctional rhythm, or atrial fibrillation.3 Care must be taken to distinguish Osborn waves from ST-elevation seen with acute myocardial infarction, which may be impossible based on ECG alone as J-waves may mimic a myocardial injury pattern. Early repolarization is considered a normal variant in individuals under age 50 when no underlying cause can be identified. Acute pericarditis presents with an entirely different history and ECG changes (ST segment elevation), which is present in most or all the precordial and limb leads.
Passive and active rewarming techniques were utilized with this patient and care was taken to handle her gently to avoid precipitating ventricular dysrhythmias. We found success with warmed intravenous fluids and a Bair Hugger device. However, had these techniques failed, other active rewarming techniques such as heated humidified oxygen, thoracic lavage, or extracorporeal membrane oxygenation may have been considered. In our case, a decision was made to withhold intubation despite the low respiratory rate, low Glasgow coma score, and hypercapnia acidosis given the potential risk of precipitating ventricular dysrhythmia with intubation.
OUTCOME
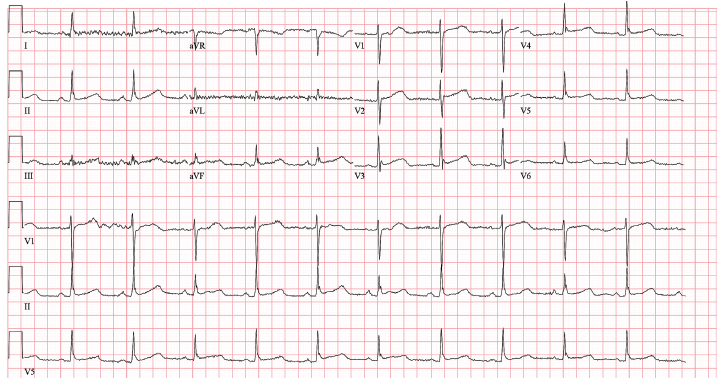
The patient was admitted to medical ICU for continued care. While in the medical ICU, passive and active rewarming using a Bair Hugger and warmed IV fluids was continued. Her core temperature gradually increased, as well as her heart rate and spontaneous respirations. She was transitioned to nasal cannula oxygen. Subsequent labs revealed a transient rhabdomyolysis (peak creatine kinase of 2927 IU/L), which was treated with IV fluids. Repeat EKG after rewarming can be seen below.
(Figure 2). Her mental status improved to baseline. Burn surgery was consulted for minor frostbite on her hands and recommended local wound care. The patient refused rehabilitation placement and she was discharged home on hospital day 4. No significant neurologic or respiratory complications were reported.
Andrew S. Wright MD, is a PGY-3 emergency resident, Case Western Reserve University/MetroHealth Medical Center in Cleveland, OH.
David Effron, MD, is assistant professor of emergency medicine at Case Western Reserve University, attending physician in the department of emergency medicine at the MetroHealth Medical Center, and consultant emergency physician at the Cleveland Clinic Foundation, all in Cleveland.
References:
1.Yan GX, Antzelevitch C. Cellular basis for the electrocardiographic J wave. Circulation. 1996;93(2):372-379.
2.Nolan J, Soar J. Images in resuscitation: the ECG in hypothermia. Resuscitation. 2005;64(2):133-134.
3.Mattu A, Brady WJ, Perron AD. Electrocardiographic manifestations of hypothermia. Am J Emerg Med. 2002;20(4):314-326.