
Childhood Obesity An Optimistic Review, Part 2: Management
Editor’s Note:
This second article of a 3-part series outlines childhood obesity treatment strategies. This first article explores how obesity is defined and offers advice about assessing BMI percentile, approaching the history and physical examination, and ordering the most appropriate diagnostic tests. Part 3 counters common myths about pediatric obesity with facts.
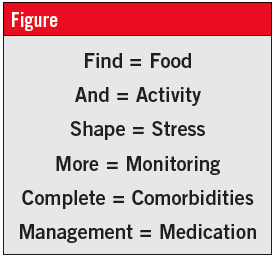 There are 6 areas of focus for the management of pediatric obesity: food, activity, stress, monitoring, comorbidities, and medication. For management to succeed in the short and long terms, plans in each of these areas must be negotiated and designed with the child and the family. I have created a mnemonic to remember the 6 areas: “Find And Shape More Complete Management” (Figure).
There are 6 areas of focus for the management of pediatric obesity: food, activity, stress, monitoring, comorbidities, and medication. For management to succeed in the short and long terms, plans in each of these areas must be negotiated and designed with the child and the family. I have created a mnemonic to remember the 6 areas: “Find And Shape More Complete Management” (Figure).
Find/Food
According to statistics from the Centers for Disease Control and Prevention, 36% of U.S. adults are obese and another 33% are overweight.1 It seems likely that at least half of these 69% of adults have tried to change the way they eat or have engaged in a formalized diet at least once. Opinions abound on what balance of macronutrients and micronutrients are essential for healthy weight loss, and on how often to eat, sleep, and exercise. While a full discussion is beyond the scope of this review, a number of uncontested facts about nutrition bear emphasis in encouraging healthy weight loss in overweight and obese children.
Find food that the child likes and that also is nutrient-dense and energy-lean. This means foods that are voluminous for their total caloric load. More volume often means more chewing and more satiety. Included in this category are fruits, vegetables, lean meats, and whole grains. Even snacks can be selected for nutrient-energy balance.2
Find drinks that the child likes and that also are energy-lean. It is easy for a child to gulp down hundreds of calories. Juice and soda pop have been vilified because of the link between intake of caloric beverages and weight gain in children. The drinks would be harmless if consumed in a reasonable amount (4 ounces of apple juice is just over 50 calories). Unfortunately, in children as in adults, lower-priced, larger-volume sweet drinks often are the beverages of choice. Instead, encourage the consumption of water, low-fat dairy drinks, or low-fat dairy-substitute drinks. The jury is out on whether artificially sweetened drinks do more harm than good, but when consumed in moderation, a diet beverage is likely to be acceptable.
 Find out what the adults can do. Not every family can cook every day, has access to fresh fruits and vegetables, and knows how to prepare foods that are nutrient-rich and energy-lean. Identify each family’s barriers to finding food that fits their child’s needs, and offer 1 or 2 suggestions at each encounter.
Find out what the adults can do. Not every family can cook every day, has access to fresh fruits and vegetables, and knows how to prepare foods that are nutrient-rich and energy-lean. Identify each family’s barriers to finding food that fits their child’s needs, and offer 1 or 2 suggestions at each encounter.
Find food for breakfast. Eating breakfast reduces a child’s likelihood of becoming obese.3 Eating breakfast not only can help with a child’s weight management, but also can help with his or her school performance.
And/Activity
Activity doesn’t only mean doing something, it also means not doing nothing. That may seem obvious, but a growing percentage of a child’s time in and out of school is sedentary. Any management approach to the obese child needs to address both increasing activity and decreasing sedentary time.
And activity. A growing body of evidence shows that while aerobic activity is needed for adult cardiovascular health, resistance/strength-training/muscle-building activities influence a child’s success in weight management and improving ill health.4 Therefore, the necessary emphasis is on building muscle. Household items (eg, cans and jars, towels, a broom with grocery bag weights tied on each end) can be used for strength and resistance training. A set of resistance bands (or bungee cords from the hardware store) can be obtained easily.
Less sedentary time. Recommendations to limit screen time to 2 hours a day are not new. Television time in overweight and obese children is specifically associated with increases in fasting glucose levels, insulin levels, and measures of insulin resistance.5 One author6 offers the following guidelines as goals to be achieved gradually: no screen time in children younger than 3 years; 30 to 60 minutes daily for children aged 3 to 7 years; 60 minutes daily for children aged 7 to 12 years; 90 minutes daily for children aged 12 to 16 years, and 120 minutes daily for children aged 16 years and older. Even if these goals are unrealistic for many families, setting intermediate goals can improve the chances of successful reduction of screen time.
Find out what the child and family can do. This is not a one-size-fits-all problem, and one solution will not work for every family. Some families will belong to health clubs, while others will have transportation problems or limited space. Negotiate a starting point and reassess over time, setting new goals as old goals are either reached or determined to be unreachable.
Shape/Stress
Stress is a part of every life. Stress isn’t good or evil, it isn’t helpful or harmful, it isn’t a motivator or an impediment. How each person manages stress is the issue. The goal is helping families assess stress in the context of a child’s life and identify and implement healthy ways to manage it. Many children and adults use food as a coping mechanism, a reward, and a stress-management tool. A recently published study7 demonstrated a relationship between cortisol, stress, BMI, and eating in the absence of hunger in children aged 8 to 9 years. Similar results have been reported in adults.
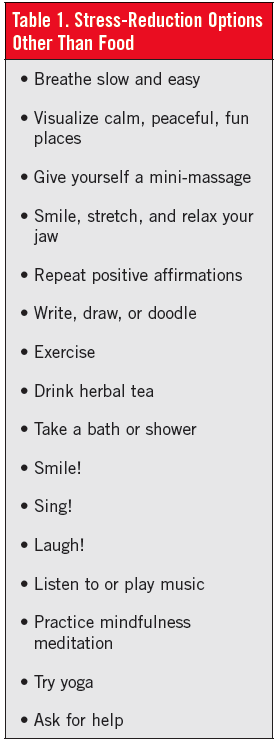
The first step to shaping stress into a less harmful experience is recognizing that stress exists and that each person has choices in how he or she responds. Help the child and family identify healthy stress-reduction options, and let them each choose the healthier alternatives they feel comfortable with (Table 1).
More/Monitoring
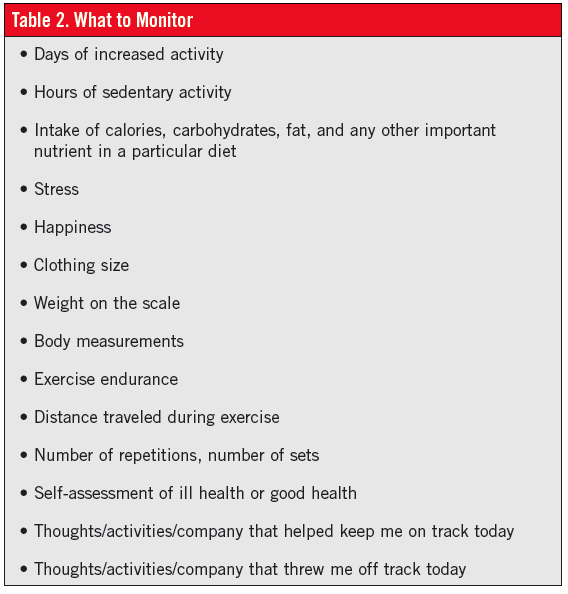
Monitoring can include foods eaten, activities done, challenges and barriers overcome, and positive behavioral changes and positive results realized (Table 2). High-tech and low-tech tools are available for monitoring. Some require online access; others are smartphone applications or written journals. Even stickers on a calendar (around $3 total cost at most dollar stores) can be useful to children and families who want to take ownership of their progress.
Complete/Comorbidities
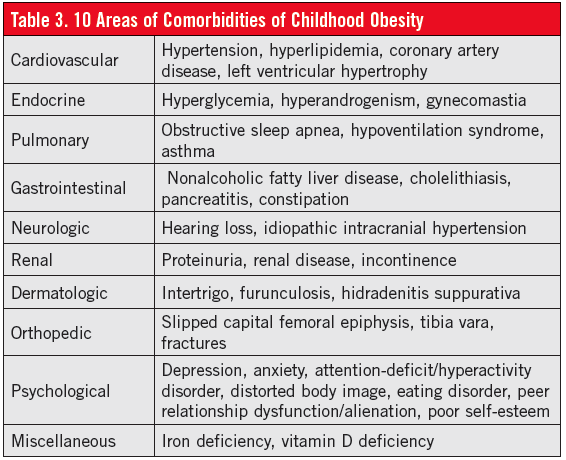
The comorbidities of childhood obesity are numerous. It seems that not a week passes without another news item about some connection between obesity and ill health. Table 3 lists comorbidities to consider assessing.
There is an art to the balance between identifying and treating comorbidities and focusing on improving health and reducing obesity and its effects on health. Too much emphasis on what’s wrong can be overwhelming for patients and can increase perceptions of hopelessness and helplessness, the enemies of optimism. Modeling an upbeat, encouraging attitude is extremely important.
Management/Medications
Medications to treat the comorbidities of childhood obesity also are numerous. Few guidelines exist about the use of pharmacologic agents as primary treatment of childhood obesity. Only one medication, orlistat, is approved by the U.S. Food and Drug Administration for the treatment of childhood obesity. Metformin has been extensively studied in the pediatric population, but its use for childhood obesity is an off-label indication. Several other less well-studied medications are used off-label for pediatric weight loss, and several are in the research stage.8-10
Orlistat is available generically and under the brand names Xenical (prescription) and Alli (lower-strength, over-the-counter). Prescription-strength orlistat is approved for use in childhood obesity for up to 1 year in patients aged 12 years and older.
Orlistat is a reversible lipase inhibitor that blocks intestinal lipid absorption, thereby increasing fecal excretion of triglycerides and cholesterol. Common side effects include oily bowel movements, flatus with discharge, and oily spotting on underwear; there also have been reports of cholelithiasis, pancreatitis, and one case of acute liver injury that has not been definitively linked to orlistat. When used in conjunction with lifestyle changes, orlistat is associated with a modest increase in weight loss. The primary drawback is acceptance of these side effects, although they tend to decrease over time.
Metformin is available generically and under a variety of brand names. It is approved for the treatment of childhood diabetes in children aged 10 years or older, and it has been used off-label in adolescent polycystic ovary syndrome, childhood premature adrenarche, and childhood obesity.
Metformin is an insulin-resistance medication that reduces hepatic glucose production, lowers insulin concentration, decreases fat-cell lipogenesis, and increases levels of glucagon-like peptide-1. Common side effects include gastrointestinal upset, headache, and myalgia; vitamin B12 deficiency and hypoglycemia also have been reported. Lactic acidosis is a very rare but severe side effect associated with metformin, but it has not been reported in a pediatric patient.11 Metformin, when used in conjunction with lifestyle changes, is associated with mild to moderate increase in weight loss.
The use of either orlistat or metformin requires ongoing monitoring.
Bariatric Surgery
Bariatric surgery increasingly is being seen as a solution to adult obesity and even adult overweight. In pediatrics, however, a limited number of centers nationwide have a comprehensive pediatric bariatric surgery program, and the rate of bariatric surgery, reported as 0.8 per 100,000 in 2000, has increased to and leveled off at 2.3, 2.2, and 2.4 per 100,000 in the years 2003, 2006, and 2009, respectively.12 In general, surgery is limited to adolescents at least 13 to 15 years old, with sexual maturity rating IV, and with a BMI of 35 to 50 kg/m2.
A compelling case can be made for adolescent bariatric surgery, including lower morbidity rates and the potential for prevention of future health problems. At least 3 deaths (not perioperative) have been reported after adolescent bariatric surgery. Most importantly, little long-term data exist about children who have undergone bariatric surgery. The multicenter Teen-Longitudinal Assessment of Bariatric Surgery (Teen-LABS) study began in March 2007 and has an estimated completion date of June 2016.13 The progress of 200 patients, aged 12 to 18 years, will be followed longitudinally.
Medical Home oR Referral
Referring a child and family to a specialist has advantages and disadvantages. Among the positive aspects are that the child with obesity and his or her family may have access to a greater range of resources, may have underlying problems identified and treated, and may be more motivated to proceed with management to avoid potential risks. The negative aspects of specialist referrals include the family’s concern that the child cannot be taken care of in your office; the time and hassle of referrals, scheduling, and commuting (often to a distant location); and the risk of feeling overwhelmed if “too many doctors” are involved. Moreover, a child’s medical home should be his or her primary care provider’s office, not a web of specialists among whom the child’s family bounces. That said, a well-considered referral is vital for the care of a child with obesity (Table 4).

Putting It All Together
At each visit, encourage the child and family to take steps toward better health, and reassess their progress (Table 5). At each follow-up, review their choices and commend accomplishments using specific descriptive language (eg, “You found that taking a deep breath really helped you avoid eating every time you felt stressed”), not general praise (eg, “Good job!” “You did great!” “Fantastic!”).
Also investigate the child’s and family’s barriers to success. What did they try that didn’t work this time? What just wasn’t possible? What interfered? What modifications can be planned together to improve results?
Why Be Optimistic?
You may believe that you simply do not have the time in your day to accomplish all of these tasks at any single patient visit. That’s OK. Pediatrics is about longitudinal follow-up, assessment, and management. No individual or society becomes obese overnight. This isn’t a quick-fix situation. Whether you have a paper chart or an electronic health record, start a checklist to review with each patient at each visit. Schedule visits at regular intervals (eg, once a month, once a quarter) to touch base with the child and the family.
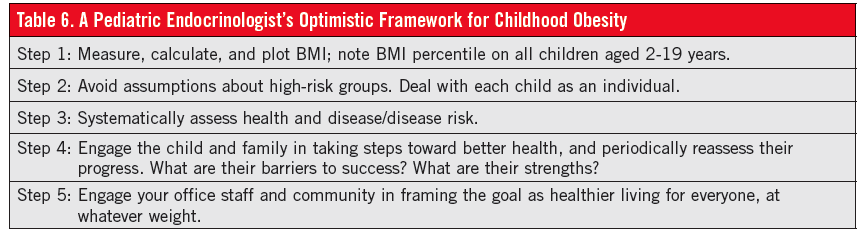
Remember that just as the children and families you treat will need to take 1 or 2 steps at a time, you’ll also need to incorporate new procedures and behaviors gradually. Don’t take on too much at once. Build slowly for long-term success (Table 6). We must optimistically and confidently focus on improving health and reducing short- and long-term complications, at all weights, for the children in our care.
References:
1.Centers for Disease Control and Prevention. Overweight and obesity. http://www.cdc.gov/obesity/data/facts.html. Updated April 27, 2012. Accessed October 3, 2013.
2.Centers for Disease Control and Prevention. Low-energy-dense foods and weight management: cutting calories while controlling hunger. http://www.cdc.gov/nccdphp/dnpa/nutrition/pdf/r2p_energy_density.pdf. Accessed October 3, 2013.
3. Antonogeorgos G, Panagiotakos DB, Papadimitriou A, Priftis KN, Anthracopoulos M, Nicolaidou P. Breakfast consumption and meal frequency interaction with childhood obesity. Pediatr Obes. 2012;7(1):65-72.
4. Ho M. Garnett SP, Baur LA, et al. Impact of dietary and exercise interventions on weight change and metabolic outcomes in obese children and adolescents: a systematic review and meta-analysis of randomized trials. JAMA Pediatr. 2013;167(8):759-768.
5. Goldfield GS, Saunders TJ, Kenny GP, et al. Screen viewing and diabetes risk factors in overweight and obese adolescents. Am J Prev Med. 2013:44(4 suppl 4):S364-S370.
6. Sigman A. Time for a view on screen time. Arch Dis Child. 2012;97(11):935-942.
7. Francis LA, Granger DA, Susman EJ. Adrenocortical regulation, eating in the absence of hunger and BMI in young children. Appetite. 2013;64:32-38.
8. Caprio S. Treating child obesity and associated medical conditions. Future Child. 2006;16(1):209-224.
9. Freemark M. Pharmacotherapy of childhood obesity: an evidence-based, conceptual approach. Diabetes Care. 2007;30(2):395-402.
10. Sherafat-Kazemzadeh R, Yanovski SZ, Yanovski JA. Pharmacotherapy for childhood obesity: present and future prospects. Int J Obes (Lond). 2013;37(1):1-15.
11. Misbin RI. The phantom of lactic acidosis due to metformin in patients with diabetes. Diabetes Care. 2004;27(7):1791-1793.
12. Kelleher DC, Merrill CT, Cottrell LT, Nadler EP, Burd RS. Recent national trends in the use of adolescent inpatient bariatric surgery: 2000 through 2009. JAMA Pediatr. 2013;167(2):126-132.
13. ClinicalTrials.gov. Teen-Longitudinal Assessment of Bariatric Surgery (Teen-LABS): adolescent bariatrics: assessing health benefits and risk. http://www.clinicaltrials.gov/ct2/show/NCT00474318. Accessed October 3, 2013.
Dr Moltz is director of pediatric diabetes services at Children’s Hospital of Michigan and an assistant professor of pediatrics at Wayne State University School of Medicine in Detroit.