
Peer Reviewed
Cerebrospinal Fluid Pseudocyst in a Toddler
A 3-year-old African American girl presented with a 1-month history of cramping abdominal pain exacerbated by defecation. The patient had a history of congenital hydrocephalus for which she had undergone ventriculoperitoneal (VP) shunt placement, along with epilepsy and associated developmental delay. Her mother also reported that the girl had had almost daily fever, with temperatures as high as 39.4°C, and a 2-kg weight loss since the onset of symptoms.
The child had been seen as an outpatient and had received a diagnosis of functional constipation. Polyethylene glycol 3350 was started, but the abdominal pain persisted despite her subsequently having soft, watery stools. A urine culture then grew pan-sensitive Escherichia coli, but the child’s cramping abdominal pain and intermittent fever continued despite receiving oral trimethoprim-sulfamethoxazole for 7 days to treat her urinary tract infection.
Of note, the patient’s VP shunt had been placed shortly after birth, and there had been no malfunction or revision. Although she had experienced occasional brief seizures at baseline, she had required intubation and pentobarbital-induced coma for status epilepticus 2 weeks prior to the onset of abdominal pain. No nidus for this episode had yet been determined, and the child had experienced no increase in seizure frequency since that time.
Upon admission, the patient was afebrile with stable vital signs. Physical examination was notable for macrocephaly and frontal bossing, with the proximal shunt catheter palpable over the right occiput; the shunt valve behind right ear was nontender. The abdomen was tense with generalized distension, although exaggerated fullness was appreciated in the left flank and epigastrium. Diffuse tenderness to light and deep palpation was evident without rebound, and no discrete mass was palpable.
Laboratory values were significant for a white blood cell count of 18,000/µL (77% granulocytes, no band forms), a hemoglobin level of 9.1 g/dL (decreased from 12.7 g/dL 1 month prior), a platelet count of 1163 × 103/µL, and an erythrocyte sedimentation rate of 101 mm/h. An abdominal radiograph obtained earlier on the date of admission demonstrated a nonobstructive gas pattern and the intact distal shunt tip (Figure 1).

Figure 1. Supine abdominal radiograph showing the intact VP shunt distal catheter tip (arrow) with accompanying nonspecific bowel gas pattern.
These findings, along with the reported persistent fever and weight loss, prompted concern for occult intra-abdominal abscess or malignancy. As such, a computed tomography (CT) scan with contrast of the abdomen and pelvis was obtained, revealing an organized, rim-enhancing fluid collection surrounding the distal shunt tip in the lower left abdomen, just anterior to the L4 vertebral body; this was compatible with cerebrospinal fluid (CSF) pseudocyst (Figure 2). The patient was then transferred to a tertiary-care facility for anticipated externalization.
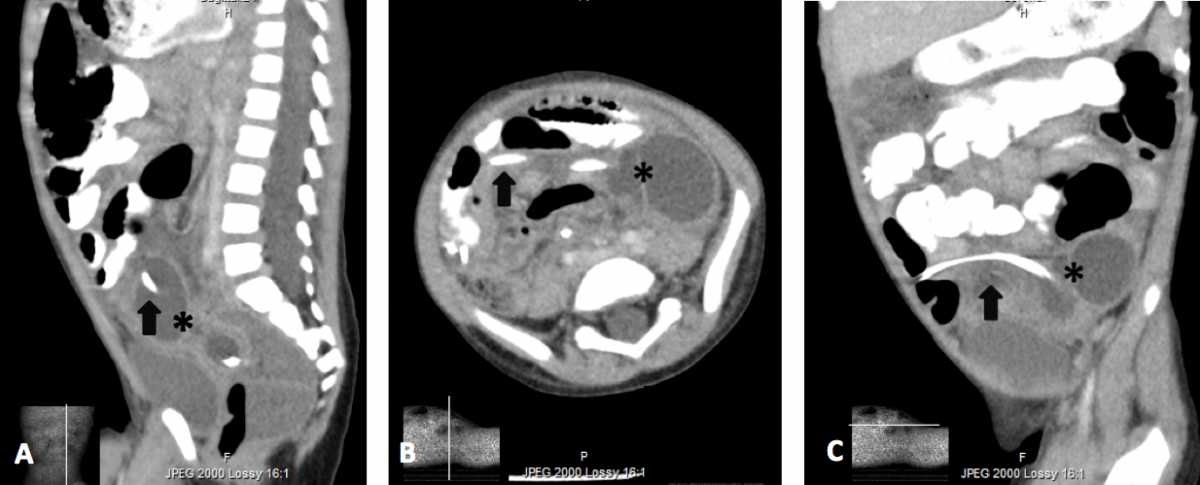
Figure 2. Sagittal (a), axial (b), and coronal (c) contrast-enhanced CT images demonstrating the distal VP shunt catheter tip (arrow) and CSF pseudocyst (*).
Discussion
Harsh first described the formation of a CSF abdominal pseudocyst as a result of VP shunt placement in 1954.1 While abdominal CSF pseudocyst is a rare complication of VP shunt placement, both proximal and distal shunt insufficiency should be considered in shunt-dependent children presenting with headache, nausea, or vomiting. Furthermore, abdominal pain or distension along with other signs of acute abdomen in a shunted child should prompt workup for CSF pseudocyst or peritonitis, since neurologic symptoms are not always present in patients with distal shunt complications.2,3
Previous case series suggest that children younger than 10 years are more likely to have secondarily infected CSF pseudocysts compared with adolescents and adults.3 Most patients who develop CSF pseudocysts have also had frequent and often recent shunt revisions.4,5 Interestingly, our patient had had no prior shunt malfunction or abdominal surgeries, making our case unique and highlighting the importance of considering this diagnostic entity in any shunt-dependent child with new-onset abdominal distension, even in the absence of prior complications.
References:
- Harsh GR III. Peritoneal shunt for hydrocephalus, utilizing the fimbria of the fallopian tube for entrance to the peritoneal cavity. J Neurosurg. 1954;11(3):284-294.
- Yuh S-J, Vassilyadi M. Management of abdominal pseudocyst in shunt-dependent hydrocephalus. Surg Neurol Int. 2012;3:146.
- Dabdoub CB, Dabdoub CF, Chavez M, et al. Abdominal cerebrospinal fluid pseudocyst: a comparative analysis between children and adults. Childs Nerv Syst. 2014;30(4):579-589.
- Rainov N, Schobess A, Heidecke V, Burkert W. Abdominal CSF pseudocysts in patients with ventriculo-peritoneal shunts: report of fourteen cases and review of the literature. Acta Neurochir (Wien). 1994;127(1-2):73-78.
- Hahn YS, Engelhard H, McLone, DG. Abdominal CSF pseudocyst: clinical features and surgical management. Pediatr Neurosci. 1985-1986:12(2):75-79.