
Peer Reviewed
Can You Identify These Knee Problems?
Klippel-Trenaunay Syndrome
Adam Martin, BS, Bridget M. Bryer Groff, MD, and Barbara B. Wilson, MD
University of Virginia School of Medicine, Charlottesville
 A 7-year-old girl presented with pain and discomfort in the left leg that was exacerbated by physical activity. She had been born with a port-wine stain on the left knee. As her mobility increased, she occasionally complained of discomfort in the left leg.
A 7-year-old girl presented with pain and discomfort in the left leg that was exacerbated by physical activity. She had been born with a port-wine stain on the left knee. As her mobility increased, she occasionally complained of discomfort in the left leg.
Klippel-Trenaunay syndrome (KTS) was diagnosed at age 3 years after an evaluation for swelling, discoloration, and pain of the left leg. Magnetic resonance angiography and venography had revealed abnormally dilated, tortuous veins in the subcutaneous tissues from the distal thigh to the posterolateral calf with involvement of the proximal anterior tibial muscle. The parents had elected for conservative management with observation.
At the patient’s current visit, she was noted to have 2 erythematous to bluish vascular plaques on the superior and inferior aspects of the patellar surface with subcutaneous nodular swellings and varicosities predominantly on the lateral aspect of the lower leg. Edema and hypertrophy of the left limb were apparent. KTS usually has no apparent racial or gender predilection, and studies show no definitive gene localization.1 The presentation varies from mild cases with a small portwine stain and few varicosities to severe cases with limb overgrowth, pain, recurrent cellulitis, thrombophlebitis, thromboembolism, and visceral bleeding from vascular malformations.2
Capillary malformations are frequently the first abnormality observed. Varicosities most often present when the child begins to walk.2 Limb length discrepancies progress at variable rates but typically stabilize around puberty.3 A variant of KTS, Parkes Weber syndrome presents with an arteriovenous fistula component.4 The workup includes imaging studies to assess the type, extent, and severity of vascular malformations. Doppler ultrasonography is the initial study of choice, although several other methods are available. Evaluation of limb length discrepancy with plain films of the long bones is recommended. MRI is helpful in evaluating soft tissue hypertrophy and may be used to determine the degree of infiltration and evaluate deeper tissues before treatment.2 Because KTS is a combined malformation syndrome, a multidisciplinary approach to management is advised.
Treatment depends on disease severity and is largely conservative, focusing on symptom relief.4 Compression therapy can alleviate venous insufficiency and lymphedema, although diuretics may be needed for significant fluid collection. Physical therapy may improve limitations secondary to limb overgrowth. For patients with a leg length difference of less than 1.5 cm, heel inserts or special orthopedic footwear may prevent vertebral scoliosis.5 Patients with a leg length discrepancy of greater than 2 cm should be referred for orthopedic surgery.5 Postoperative anticoagulation should be considered in patients with KTS because they are at higher risk for thrombotic complications.4 Similarly, female patients with KTS are generally advised to avoid oral contraceptives because of their prothrombotic potential.4
Patients with complications, such as infection and thrombus formation (including pulmonary emboli), require appropriate treatment and evaluation for more aggressive intervention. For patients who do not respond to conservative approaches or who desire more definitive results, other therapies are available. Port-wine stains may be treated with pulsed dye lasers.4 Venous sclerotherapy, stripping, or ligation may be used to treat symptomatic malformations, although recurrence is common.2 For this child, we recommended custom-fit hose with 30 mm Hg compression. She was referred tointerventional radiology for consideration of embolization or surgery and to orthopedics for treatment of limb length discrepancy. The psychological impact of the physical deformity should not be overlooked. We encouraged this patient and her family to participate in a support group.
REFERENCES:
- Oduber CE, van der Horst CM, Hennekam RC. Klippel-Trenaunay syndrome: diagnostic criteria and hypothesis on etiology. Ann Plast Surg. 2008;60: 217-223.
- Gloviczki P, Driscoll DJ. Klippel-Trenaunay syndrome: current management. Phlebology. 2007;22: 291-298.
- Jacob AG, Driscoll DJ, Shaughnessy WJ, et al. Klippel-Trénaunay syndrome: spectrum and management. Mayo Clin Proc. 1998;73:28-36.
- Kihiczak GG, Meine JG, Schwartz RA, Janniger CK. Klippel-Trenaunay syndrome: a multisystem disorder possibly resulting from a pathogenic gene for vascular and tissue overgrowth. Int J Dermatol. 2006;45:883-890.
- Gloviczki P, Hollier LH, Telander RL, et al. Surgical implications of Klippel-Trenaunay syndrome. Ann Surg. 1983;197:353-362.
NEXT: Lymphangioma Circumscriptum
Lymphangioma Circumscriptum
Robert P. Blereau, MD
This lesion on her knee had been present for 5 years, reported a 22- year-old woman. It was not related to any trauma; its size had not changed, but occasionally it became darker or lighter.

Excisional biopsy revealed lymphangioma circumscriptum—a benign, hamartomatous malformation of dilated lymph channels that may be filled with clear fluid because of communication with deeper lymphatics or, as in this case, serosanguinous fluid.
Treatment (excisional biopsy) is indicated primarily for diagnosis, cosmetic reasons, and relief of patient anxiety, writes Dr Robert P. Blereau of Morgan City, La, but it also prevents leakage of fluid and infection. The deep communicating lymphatic cistern must also be excised, otherwise lesions likely will recur.
NEXT: Occupational Prepatellar Bursitis
Occupational Prepatellar Bursitis
Shailendra K. Saxena, MD, PhD, Renee Dentlinger, Emily Siedlik, and Mikayla Spangler
For 2 months, a 29-year-old man had pain and circular, soft swelling (7 × 7 cm in diameter) over the anterior left knee, superficial to the patellar ligament. Pain was minimal and associated with extension and flexion (A and B).

For the past 10 years, the patient had been employed laying floor tile. A history of repetitive kneeling coupled with the pain on inspection and palpation of the bursa confirmed a diagnosis of prepatellar bursitis.
Prepatellar bursitis (also known as housemaid’s knee) is an inflammation of the knee bursa located between the patella and the overlying skin that presents with swelling but minimal discomfort.1,2 It is usually caused by trauma or friction from repetitive kneeling.

Management includes aspiration and drainage of bursa fluid, followed by the application of a compression wrap to the knee.3 Patients should be encouraged to avoid trauma and repetitive kneeling. The bursa fluid should be sent for culture, Gram stain, and evaluation for crystals and white blood cells. A corticosteroid injection may be considered for patients with recurrent or chronic bursitis. X-ray films of the knee are not required for a diagnosis and seldom affect management.
Most patients respond to aspiration and NSAIDs, as was the case with our patient. However, 5% to 10% of patients do not respond to conservative treatment and may require bursectomy.4 If kneeling cannot be avoided, it is recommended that patients use a kneeling pad or cushioned knee protectors and take short, periodic breaks. They may also apply ice to the area for 20 minutes, 3 or 4 times a day, as needed for pain. If the problem persists, a different profession that does not require repetitive kneeling may be considered.
REFERENCES:
- Anderson BC. Office Orthopedics for Primary Care: Diagnosis and Treatment. 2nd ed. Philadelphia: WB Saunders Co; 1999.
- Jackson JL, O’Malley PG, Kroenke K. Evaluation of acute knee pain in primary care. Ann Intern Med. 2003;139:575-588.
- Dawn B, Williams JK, Walker SE. Prepatellar bursitis: a unique presentation of tophaceous gout in normouricemic patient. J Rheumatol. 1997;24: 976-978.
- Ogilvie-Harris DJ, Gilbart M. Endoscopic bursal resection: the olecranon bursa and prepatellar bursa. Arthroscopy. 2000;16:249-253.
NEXT: Runner With Painful Swelling Behind Knee
Runner With Painful Swelling Behind Knee
David Effron, MD
For several days, a 38-year-old man has had an increasingly painful swelling behind the right knee. He runs several times a week. He has hypertension but no history of trauma or periods of inactivity, and no chest discomfort or shortness of breath. He drinks alcohol occasionally but does not use tobacco or illegal drugs.

Examination reveals a swollen soft tissue mass in the posterior popliteal fossa and an intact popliteal pulse. Sensation is intact; range of motion is minimally reduced with knee flexion. There is no erythema or warmth.
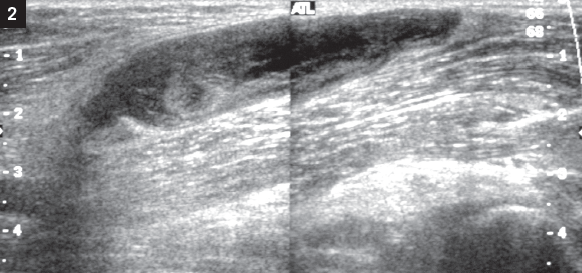
Vascular ultrasonography (Figure 2) revealed a Baker (popliteal) cyst, the most common mass of the popliteal fossa. First described in 1877 by Dr William Baker, this synovial cyst results from fluid distention of the gastrocnemius-semitendinosus bursa. Baker cysts lie between the tendons of the medial head of the semimembranous and gastrocnemius muscles, posterior to the femoral condyle. These cysts affect both sexes and all races. Although they are sometimes seen in children, especially those with juvenile rheumatoid arthritis or trauma, they typically affect adults.
The most common presenting symptoms are a popliteal mass or swelling, aching, and knee effusion. Patients may also report buckling, cracking, or locking of the knee. Associated conditions include the arthritides (such as osteoarthritis, rheumatoid arthritis, gout, and systemic lupus erythematosus); infection (tuberculosis and septic arthritis); long-standing dialysis; and internal derangement (anterior cruciate or meniscal tears and osteochondral fractures).
Potential complications of Baker cyst include rupture or dissection (pseudothrombophlebitis syndrome), DVT, infection, pulmonary embolism, leakage, and posterior compartment syndrome.
The diagnosis may be confirmed by ultrasonography, CT, arthroscopy, or MRI. Treatment involves assisted weight bearing, anti-inflammatory agents, and ice. Arthroscopy is useful for internal derangements of the knee.
The principal signs and symptoms of DVT are unilateral leg edema, leg pain or tenderness, and warmth or erythema over the area of thrombosis. Risk factors include trauma, vasculitis, medications, and a number of medical conditions. DVT may be diagnosed with duplex ultrasonography, impedance plethysmography, nuclear medicine imaging studies, or MRI.
About 0.2% to 11% of patients with Baker cyst have coexisting DVT. Therefore, DVT must be ruled out in patients who are undergoing ultrasonography to identify a possible Baker cyst.
Popliteal aneurysms are the most common peripheral aneurysms. Although the cause is unknown, they are thought to be related to trauma or atherosclerosis. Historically, such aneurysms were believed to be associated with syphilitic, mycotic, or traumatic events. Popliteal aneurysms are bilateral in 50% to 70% of cases and occur in 0.01% of hospitalized patients.
Distal embolization or aneurysmal thrombosis may produce symptoms of popliteal occlusion or claudication. However, patients are often asymptomatic at the time of diagnosis. Popliteal aneurysms typically affect persons in their 50s or 60s; most patients present with a pulsatile mass or soft tissue swelling in the popliteal fossa. Diagnosis is confirmed with duplex ultrasonography or angiography. Vascular bypass is the treatment of choice; amputation may be necessary.
A gastrocnemius tear often results from an acute, forceful push-off with the foot. Although this injury may occur with any activity, it is seen most frequently with hill running, tennis, and jumping. The intermittently active athlete ("weekend warrior") is prone to this disorder. Patients are typically men in their fourth to sixth decade of life.
Presenting symptoms include a feeling that something is "stuck" in the calf; an audible pop in the calf; pain in the calf that radiates to the ankle or knee; or swelling of the leg, including the foot or ankle. Examination often reveals tenderness on palpation of the gastrocnemius muscle, asymmetric calf swelling and discoloration, and a defect in the medial gastrocnemius muscle if the swelling has resolved.
A gastrocnemius tear is diagnosed clinically. Radiographic imaging and laboratory evaluation are reserved for investigation of other possible causes of the physical findings.
REFERENCES:
- Baker WM. On the formation of synovial cysts in the leg in connection with disease of the knee joint. St Bartholomew's Hosp Rep. 1877;13:245-261.
- Glazer JL, Hosey RG. Soft-tissue injuries of the lower extremity. Prim Care. 2004;31:1005-1024.
- Langsfeld M, Matteson B, Johnson W. Baker's cysts mimicking the symptoms of deep vein thrombosis: diagnosis with venous duplex scanning. J Vasc Surg. 1997;25:658-662.
NEXT: Blount Disease
Blount Disease
Robert P. Blereau, MD, and Timothy Haley
A 16-year-old African American boy presented with exertional pain below his left knee that severely limited his ability to participate in sports. The patient had had bilateral bowed legs until his early school years, when the right knee straightened. For the past year, exertional pain had been present below the left knee in the epiphyseal area.

Tibia vara, otherwise referred to as Blount disease, is responsible for the bowing of the patient’s left lower leg. The radiographs reveal beaking of the metaphysis and calcification and widening of the proximal tibial epiphyseal plate medially, which has produced a varus deformity at the knee.
Blount disease causes bowing at the proximal tibia that affects only the proximal tibial epiphysis. The disorder is found primarily in obese or large black children and adolescents who begin walking early, which creates excessive force on the medial physis of the proximal tibia and inhibits the normal growth of this segment. The lateral physis continues to grow normally, thereby producing the bowing at the knee.

The bowing may be unilateral or bilateral. Refer patients with Blount disease for an orthopedic evaluation. Treatment of tibia vara depends on the age of the patient and stage of the disease. Bracing and surgery may be appropriate for younger children; adolescents usually require operative intervention.
This patient had osteotomies of the tibia and fibula with internal fixation. Results of the surgery were good.