
Applying Lipid Guidelines in Daily Practice
Saturday, October 19 at 10:30 am and 11:30 am
LAS VEGAS—If you’re wondering which biomarkers you should use in assessing cardiovascular risk and when you should use them, then you might want to attend “Applying Lipid Guidelines to Daily Practice: A Focus on Risk Stratification.”
In tomorrow’s workshop, Peter H. Jones, MD, FACP, FNLA, will discuss how to implement recent guidelines that provide risk stratification algorithms to maximize cardiovascular protection without overprescribing or setting unrealistic therapeutic goals.
“Appropriate assessment for the future risk of cardiovascular disease is crucial,” says Jones, associate professor at Methodist DeBakey Heart and Vascular Center at Baylor College of Medicine in Houston, Texas. “Determining whether the patient is high-risk primary prevention or is secondary prevention (known CVD or CHD equivalent) provides guidance on prescribing long-term statin use.”
Evidence-based outcomes trials in high-CVD risk patients support the use of optimal statin dosing for its reduction in events and all-cause mortality, with a very low incidence of side effects. “Statins are first-line lipid therapy for CHD prevention and are combined with targeted healthy lifestyle habits (diet, exercise, weight control, and nonsmoking)—not to be used in place of these habits,” he says.
The target of the statin benefit is a reduction in atherogenic particle number, of which LDL-C has been a good biomarker. “However, LDL-C is not the best marker of atherogenic particle number and hence, the use of non-HDL-C, apo B, or LDL-P measures may be better for some patient groups, such as those with diabetes and those with metabolic syndrome,” Jones says.
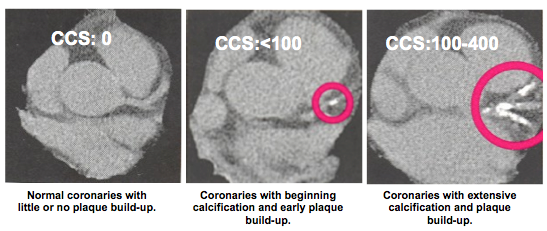
While you may be tempted to order all possible biomarkers of CVD risk or to employ imaging techniques, it’s not always necessary—especially in primary prevention cases. Jones recommends using this sort of advanced testing selectively to individualize the decision to initiate intensive therapies.
In selected patients with premature CHD or with a family history of premature CHD, measuring Lp(a) is useful since an elevation is genetically determined. The only nonlipid biomarker validated in risk assessment for statin treatment is hs-CRP in primary prevention men above age 50 and women above age 60. “Although there are other nonlipid biomarkers that can be measured, it is not clear if those really assist in identifying a higher risk than a Framingham Risk Score would tell you,” Jones says.
Addressing additional lipid and non-lipid novel markers might enhance CVD risk identification and possibly predict risk reduction; however, the benefit and any cost effectiveness remains to be established.
— Colleen Mullarkey