
Worsening Dizziness in an Elderly Man
An 85-year-old man presents to the emergency department (ED) with fatigue and dizziness of several weeks’ duration; these symptoms have worsened during the past 2 hours. He has not had any frank syncope, chest pain, or palpitations. He is normally active and plays singles tennis every day but has not had sufficient energy to play for the past 2 weeks. He denies any fever or headache. He denies any modifying factors; he has not noticed any orthostatic relationship to his symptoms or any change with head motion. He has limited cervical spine mobility as a result of a vertebral fusion he underwent 20 years ago for degenerative disc disease. His medical history is notable for a myocardial infarction 20 years earlier, for which he was treated with streptokinase while visiting Belgium; hypertension; prostate cancer (in remission); hypothyroidism; gastroesophageal reflux disease; and osteoarthritis.
This thin but otherwise well-nourished man is in no acute distress. His temperature is 35.6°C (96.1°F); heart rate, 45 beats per minute and regular; respiration rate, 16 breaths per minute; and blood pressure, 147/78 mm Hg lying, 157/85 mm Hg standing. His head and neck examination is normal with no carotid bruits and no jugular venous distension. Lungs are clear. Cardiac examination reveals no murmurs, rubs, or gallops. Results of the abdominal examination are benign; his lower extremities have symmetric trace pedal edema.
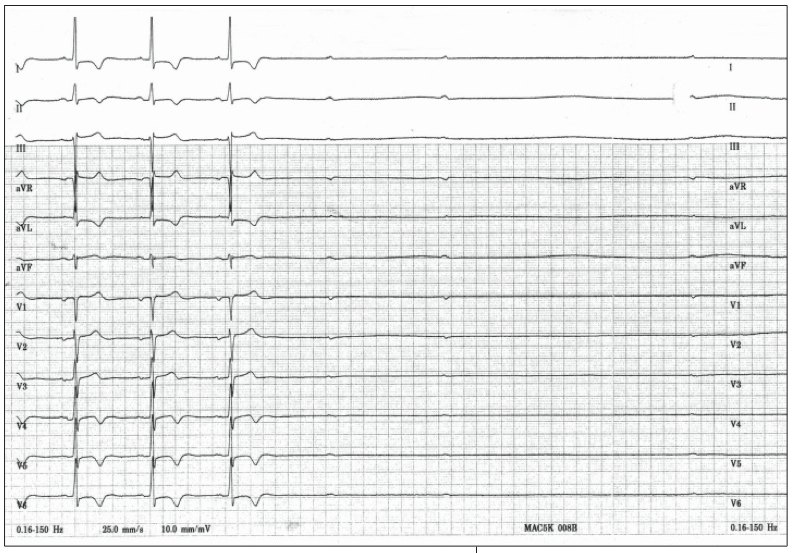
In the ED, carotid massage is performed to determine whether the patient’s symptoms can be reproduced. The 12-lead rhythm strip recorded during carotid massage is shown here.
Which of the following best explains the ECG findings?
A. Complete heart block
B. Sinus arrest and complete heart block with carotid sinus hypersensitivity
C. Severe sinus arrhythmia
D. Ectopic atrial focus
E. Artifact/loose ECG lead
(Answer and discussion begin on next page.)
Answer: B, Sinus arrest and complete heart block with carotid sinus hypersensitivity
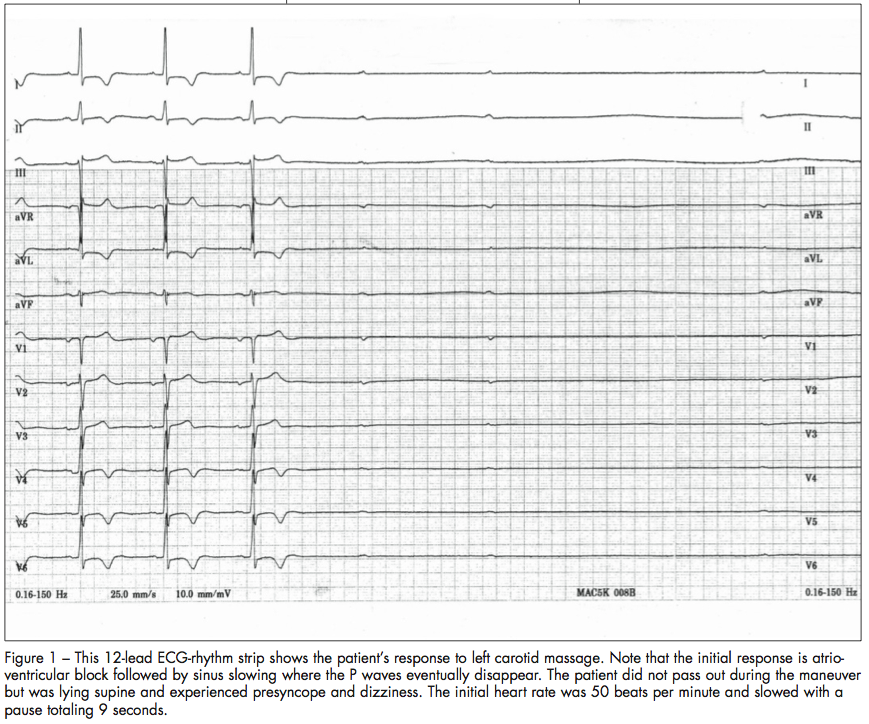
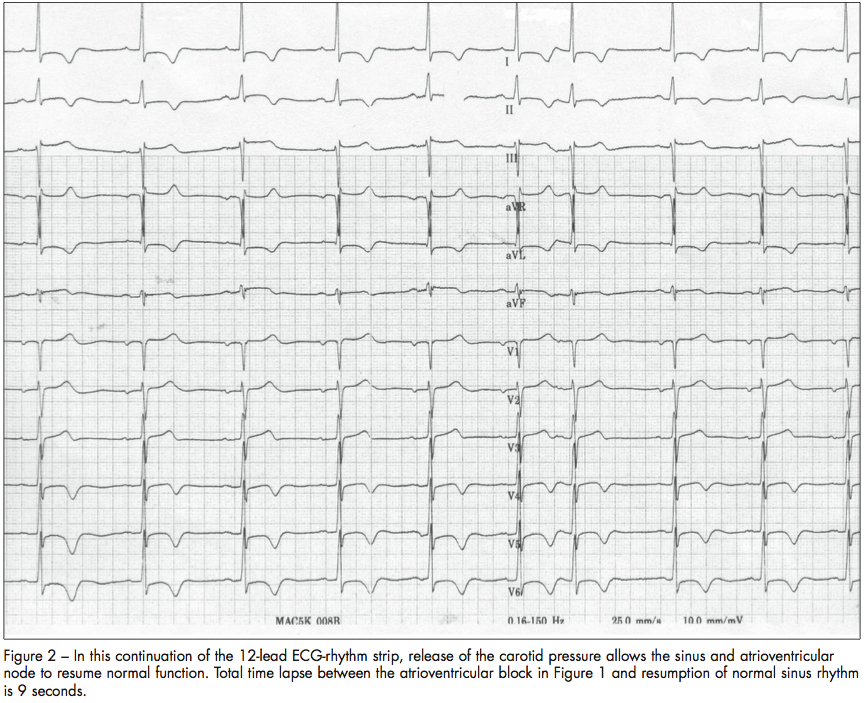
This patient experiences high-grade atrioventricular conduction block during the carotid massage resulting in lack of conduction to the ventricle, but the sinus node eventually stops as well making complete heart block (choice A) an incomplete answer. While this patient does have slight irregularity in the beats leading up to the carotid massage, sinus arrhythmia (choice C) does not explain the long 9-second pause that is seen (Figure 1). Before the pause, the rhythm strip shows slowing and eventual cessation of sinus P wave activity, making limb lead loss unlikely (choice E). Prior to the pause, the patient has normal sinus rhythm (Figure 2) making ectopic atrial focus (choice D) an incorrect answer.
PATHOPHYSIOLOGY OF CAROTID SINUS HYPERSENSITIVITY
The hallmark of autonomic nervous system disorders is an inappropriate response of the autonomic system to a stimulus, which can lead to orthostatic intolerance with such symptoms as dizziness and, in more extreme cases, syncope. Not all autonomic nervous disorders have an orthostatic component, and other stimuli may be able to trigger the same untoward symptoms. Some of these inappropriate syndromes include reflex/situational syncope (often blamed for micturition syncope), vasovagal syncope, postural orthostatic tachycardia syndrome, and carotid sinus hypersensitivity (CSH).
CSH is an exaggerated response to carotid sinus stimulation, which includes the carotid massage that was performed in this patient’s case. The underlying mechanism involves activation of the baroreceptors in the carotid sinus in the neck and can be triggered by head turning, shaving, or wearing a tight collar. In this instance, the symptoms were reproduced by applying gentle manual pressure to the left carotid sinus.
CSH can be classified into 3 groupings that describe the etiology of the mechanism1:
•Vasodepressor with a drop in blood pressure (if systolic blood pressure drops by more than 50 mm Hg with stimulus).
•Cardioinhibitory with associated bradycardia (if there is greater than a 3-second pause with stimulus).
•Mixed with both bradycardia and drop in blood pressure.
CSH is most commonly found in persons older than 50 years old and has been estimated to exist in as many as 45% of elderly patients with recurrent syncope or otherwise unexplained falls.2 Cardiac pacing therapy has been an effective tool to prevent recurrent syncope in patients with cardioinhibitory CSH, and current American College of Cardiology/American Heart Association guidelines recommend considering a pacemaker for those who have symptoms consistent with CSH and who have documented pauses from sinus arrest or atrioventricular block lasting at least 3 seconds.3
OUTCOME OF THIS CASE
The patient was admitted to the telemetry service and underwent implantation of a dual chamber pacemaker with DDD pacing. The patient recovered quickly and was back playing singles tennis in a short time with no further dizziness or presyncope.
1. Kusumoto FM, Goldschlager NF. Cardiac Pacing for the Clinician. Philadelphia: Lippincott Williams & Wilkins; 2001:261-266.
2. Richardson DA, Bexton RS, Shaw FE, et al. Prevalence of cardioinhibitory carotid sinus hypersensitivity in patients 50 years or over presenting to the accident and emergency department with “unexplained” or “recurrent” falls. PACE. 1997;20:820-823.
3. Kenny RA, Bexton RS, Steen NI, et al. Cardiac pacing reduces falls in carotid sinus hypersensitivity: the SAFE-PACE trial. J Am Coll Cardiol. 2000;35:
142A.