
What Is This Man’s Oral Risk Factor for Haemophilus Endocarditis?
 For 5 days, a 30-year-old man has had fever, rigors, and diaphoresis. He admits to intravenous (IV) cocaine use.
For 5 days, a 30-year-old man has had fever, rigors, and diaphoresis. He admits to intravenous (IV) cocaine use.
His temperature is 38.6°C (101.4°F); pulse, 108 beats per minute (regular); respiration rate, 18 breaths per minute (unlabored); and blood pressure, 120/70 mm Hg. There are no peripheral signs of endocarditis (petechiae, conjunctival hemorrhages, Janeway’s or Osler’s lesions, or splinter hemorrhages or Roth’s spots on funduscopic examination). He has good dentition, no oral lesions, and a normal tongue that is not pierced; no nasopharyngeal abnormalities are noted.
His cardiac examination demonstrates a slightly enlarged left ventricle to palpation and a prominent IV/VI holosystolic murmur, maximum at the fourth left intercostal space, transmitting to the mid-axillary line and posterior chest. Jugular venous distension and right ventricular abnormalities are absent. The results of neurological, pulmonary, abdominal, skin, and joint examinations are unremarkable.
Pertinent laboratory data include a hemoglobin level of 10.4 g/dL; white blood cell count, 44,900/µL with a differential of 72% neutrophils without bands or earlier forms; and platelet count, 160,000/µL. Sodium level is 128 mmol/L; potassium, 4.7 mmol/L; chloride, 99 mmol/L; blood urea nitrogen, 10 mg/dL; creatinine, 0.72 mg/dL; and glucose, 115 mg/dL. Calcium, magnesium, and phosphate levels are normal. Total protein and albumin levels are 5.9 and 1.8 g/dL, respectively. Bilirubin, alkaline phosphatase, and aminotransferase levels and urinalysis results are unremarkable. HIV testing is negative. Lumbar puncture reveals no abnormalities.
An ECG demonstrates only sinus tachycardia. A chest radiograph shows a small right pleural effusion that is not aspirated because of its size.
Because this patient has fever, chills, a history of IV drug use, and a prominent “new” murmur, the major diagnostic concern is acute bacterial endocarditis. Blood cultures are positive for beta-lactamase negative Haemophilus parainfluenzae sensitive to ceftriaxone.
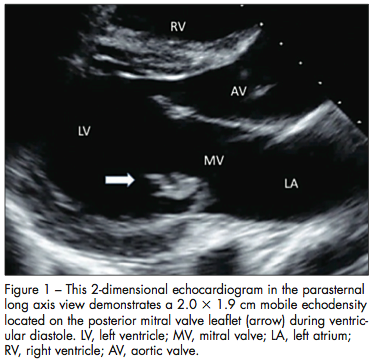
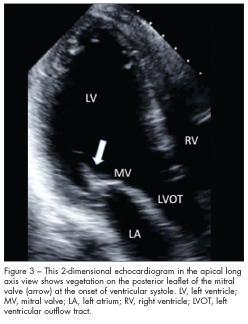
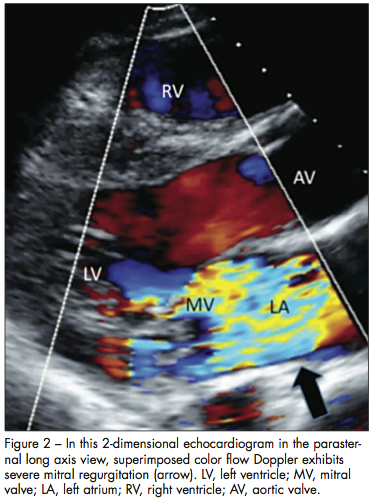 Echocardiographic images are obtained (Figures 1, 2, and 3). They demonstrate severe mitral regurgitation with a mobile, echogenic density on the posterior leaflet of the mitral valve (2.0 by 3 1.9 cm).
Echocardiographic images are obtained (Figures 1, 2, and 3). They demonstrate severe mitral regurgitation with a mobile, echogenic density on the posterior leaflet of the mitral valve (2.0 by 3 1.9 cm).
During the next few days, despite antibiotic therapy, severe mitral regurgitation leads to heart failure. The patient complains of shortness of breath at rest, lung examination results are consistent with pulmonary edema, there is new evidence of jugular venous distension, and blood pressure is decreased (systolic, 100 mm Hg).
He undergoes a mitral valve replacement with an Onyx 25/33 prosthetic valve. He tolerates the surgery well, experiences no postoperative complications, and is discharged home on postoperative day 7.
H parainfluenzae, a member of the so-called “HACEK” group, is part of normal oral and nasopharyngeal flora. It is usually implicated as a cause of infectious endocarditis in persons with poor dentition or after oral surgical procedures, but infection may also occur with IV drug use.1
 This patient had no obvious dental problems or recent oral instrumentation. How did he acquire a valvular infection with H parainfluenzae?
This patient had no obvious dental problems or recent oral instrumentation. How did he acquire a valvular infection with H parainfluenzae?
A. He has an occult tooth abscess.
B. He had a tongue piercing.
C. He licks his needles before injecting drugs.
D. He scrapes his tongue to alleviate halitosis.
(Answer on next page)
Answer: C, Needle licking before drug injection
Although Haemophilus species are a rare cause of infectious endocarditis, cases that involved H parainfluenzae infection after tongue piercing or scraping for halitosis have been reported.2,3 H parainfluenzae infectious endocarditis developed in a 26-year-old man 2 weeks after a metallic barbell-shaped stud was placed in his maxillary-labial frenulum. He had neither a history of oral procedures nor significant dental pathology.
Among IV drug users, H parainfluenzae was implicated in polymicrobial infectious endocarditis in a patient who licked her needles before injecting drugs.4 In a previous study, 28% of the subjects reported licking their needles prior to drug injection.4
A more recent study specifically addressed the logistics of needle licking in IV drug users.5 Thirteen of the forty subjects who admitted to IV drug use were interviewed and said that they licked their needles. Reasons included ritualistic practices, an attempt to “clean the needle,” an effort to enjoy the drug’s taste, a final “check” on drug quality (concentrated or dilute), and/or assessment of needle condition. In this regard, a quote from an interviewee in the study was informative: “A great way to lower your chances of overdose is by snorting or smoking instead of injecting. If you do inject, try a small taste first to judge the strength of the mix” (authors’ italics).5
1. Choi D, Thermidor M, Cunha B. Haemophilus parainfluenzae mitral prosthetic valve endocarditis in an intravenous drug abuser. Heart Lung. 2005;34:
152-154.
2. Friedel JM, Steblik J, Desai M, et al. Infective endocarditis after oral body piercing. Cardiol Rev. 2003;11:252-255.
3. Redmond AM, Meiklejohn C, Kidd TJ, et al. Endocarditis after use of a tongue scraper. Emerg Infect Dis. 2007;13:1440-1441.
4. Dieckhaus KD, Hill DR. Polymicrobial endocarditis with Haemophilus parainfluenzae in an intravenous drug user whose transesophageal echogram looked normal. CID. 1998;26:1245.
5. Deutscher M, Perlman DC. Why some drug users lick their needles: a preliminary survey. Int J Drug Policy. 2008;19:342-345.