
What is causing this 9-year-old to limp?
 HISTORY
HISTORY
A 9-year-old boy presents with a 10-day history of left leg pain and limp. The pain waxes and wanes, and it increases with ambulation. The limp worsens with activity. The boy plays soccer but has no history of specific trauma to his leg.
PHYSICAL EXAMINATION
The boy is afebrile with stable vital signs. There is no guarding with activities in the examination room, but there is mild pain with internal rotation of the left hip. There is no swelling or bruising, and the results of the left knee examination are normal.
IMAGING RESULTS
Anteroposterior and frog-leg radiographs demonstrate a well-defined, intramedullary, cystic lesion within the left femoral neck measuring 2.5 cm by 3.9 cm without periosteal reaction.
WHAT’S YOUR DIAGNOSIS?
(Answer on next page)
The patient was referred to a pediatric orthopedist and advised to avoid sports, but he was allowed to walk with the instruction to seek emergency treatment if a fall or twist occurred.
Two days later, the boy was seen in the orthopedic clinic. A more thorough history taking revealed that he had started limping 2 years earlier, but the limp had greatly worsened during the past few weeks.
 On examination, the patient had no limp, and lower extremity length and alignment were equal and symmetric. The hips had full and symmetric flexion, extension, and abduction. Trace pain at the left hip was elicited at full abduction as well as at extremes of prone hip rotation, but rotation range was symmetric. The patient was able to heel and toe walk, and he could single leg balance and hop.
On examination, the patient had no limp, and lower extremity length and alignment were equal and symmetric. The hips had full and symmetric flexion, extension, and abduction. Trace pain at the left hip was elicited at full abduction as well as at extremes of prone hip rotation, but rotation range was symmetric. The patient was able to heel and toe walk, and he could single leg balance and hop.
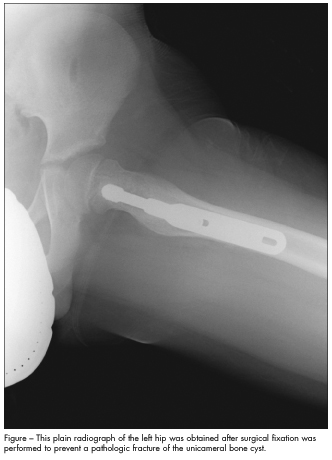
Based on the size of the lesion and its location at the femoral neck, fixation was recommended to prevent a pathologic fracture, as well as curettage and allograft to eradicate the cyst. A pathological specimen obtained at the time of surgery showed benign fibro-osseous tissue consistent with unicameral bone cyst (UBC).
At follow-up 1 month later, the boy had no pain, could ambulate without crutches, and could bear all his weight on his left leg for a few seconds. A radiograph showed a barely visible cyst outline with good homogeneity throughout the femur (Figure). He was allowed to return to all activities 2 months after surgery.
CLINICAL FEATURES
UBCs are benign, fluid-filled, single-chambered lesions that usually occur in the proximal humerus or femur of children and adolescents.1 The typical clinical presentation is a child with pain, limp, or other abnormality in the use of the affected extremity, but many patients (75%) present with a pathologic fracture thought to be secondary to weakening of the bone.2,3 The work-up should include a full history including any relevant past medical history as well as a family history of rheumatologic conditions, bone tumors, fractures, or endocrine disorders.4 The physical examination should center on the axial skeleton, and all extremities should be inspected. It is important to check for inguinal or axillary lymphadenopathy to help rule out malignancy or infection.
RADIOLOGIC FINDINGS
The typical radiographic appearance of a UBC on a plain film is a well-defined osteolytic lesion that is solitary, intramedullary, centrally located, moderately expansile, and radiolucent with a thin cortex.5 Most UBCs can be diagnosed on the basis of location, because greater than 90% occur in the proximal humerus and femur; the alternative diagnoses such as aneurysmal bone cysts, malignant osteolytic lesions, and osteomyelitis do not tend to occur in these regions.6,7
After a pathologic fracture, a portion of the wall may migrate to the dependent portion of the cyst, the so-called “fallen fragment sign,” which is pathognomonic of UBCs and can be seen on a radiograph or a CT scan.6 If a pathologic fracture is more than 2 weeks old, peri-osteal reaction may be present. If periosteal reaction is present in a radiograph obtained less than 2 weeks after the onset of symptoms, then alternative diagnoses such as tumor or infection must be explored.3 Cross-sectional CT imaging of a UBC may show homogeneity of intra-osseous contents and cortical attenuation.
TREATMENT
Asymptomatic UBCs can resolve spontaneously as the patient approaches skeletal maturity, but 85% to 93% of symptomatic lesions (those causing pain or pathologic fracture) do not resolve, thus necessitating surgical intervention.1 Indications for surgery include cysts that are progressively growing and lesions that are painful or large and at risk for pathological fracture. Treatment options include serial corticosteroid injections, bone marrow injections, and curettage and grafting with and without instrumentation, including newer minimally invasive techniques.8
Because the recurrence rate after initial surgical treatments is 15% to 40%,9 monitoring must be continued until complete resolution. Additional surgery may be indicated if a recurrent lesion grows to pose the risk of fracture. The recurrence rate after second procedures is less than 5%.10 n
1. Sung AD, Anderson ME, Zurakowski D, et al. Unicameral bone cyst: a retrospective study of three surgical treatments. Clin Orthop Relat Res. 2008;466:2519-2526.
2. Ortiz EJ, Isler MH, Navia JE, et al. Pathologic fractures in children. Clin Orthop Relat Res. 2005;432:116-126.
3. Biermann JS. Common benign lesions of bone in children and adolescents. J Pediatr Orthop. 2002;22(2):268-273.
4. Mehlman CT. Unicameral bone cyst. Available at: http://emedicine.medscape.com/article/1257331-overview. Accessed on December 6, 2011.
5. Killeen KL. The fallen fragment sign. Radiology. 1998;207(1):261-262.
6. Lokiec F, Wientroub S. Simple bone cyst: etiology, classification, pathology, and treatment modalities. J Pediatr Orthop B. 1998;7(4):262-273.
7. Agrawal R, Kizilbash S. Unexpected finding in young girl after arm injury. Consultant for Pediatricians. 2011;10(3):85-86.
8. Hou HY, Wu K, Wang CT, et al. Treatment of unicameral bone cyst: a comparative study of selected techniques. J Bone Joint Surg Am. 2010;92(4):855-862.
9. Donaldson S, Wright JG. Recent developments in treatment for simple bone cysts. Curr Opin Pediatr. 2011;23(1):73-77.
10. Mik G, Arkader A, Manteghi A, Dormans JP. Results of a minimally invasive technique for treatment of unicameral bone cysts. Clin Orthop Relat Res. 2009;467(11):2949-2954. Epub 2009 Aug 4.