
Systemic Nickel Hypersensitivity From a Swallowed Coin
 A 10-year-old boy was brought for evaluation of a spreading, intensely pruritic erythroderma of 6 days’ duration. The mother, a nurse, reported that the child had intermittent low-grade fever and 1 episode of vomiting and poor appetite, but no cough or other antecedent constitutional symptoms.
A 10-year-old boy was brought for evaluation of a spreading, intensely pruritic erythroderma of 6 days’ duration. The mother, a nurse, reported that the child had intermittent low-grade fever and 1 episode of vomiting and poor appetite, but no cough or other antecedent constitutional symptoms.
The history included no new medications or changes in household products. The child had eaten various baked goods purchased at an elementary school sale on the day the dermatitis appeared; he also had been handling metal washers as part of an experiment in his science class that day. The mother recalled that as a baby, he had significant dermatitis caused by metal snaps in clothing. She subsequently avoided similar exposure, without further incident.
The patient appeared uncomfortable on examination. His temperature was 38°C (100.4°F); other vital signs were normal. The eruption consisted of edematous papules and papulovesicles that were especially prominent on the extremities and that coalesced into confluent edematous macules and plaques over the face and trunk (Figure 1). There was intense desquamation over the flank and intertriginous areas.
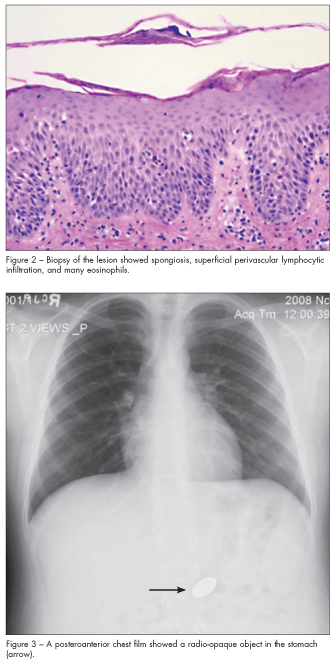
Results from skin biopsies revealed acute spongiotic dermatitis with superficial perivascular, lymphocyte-predominant mixed inflammation and many eosinophils, consistent with allergic contact dermatitis (Figure 2).
Results from a throat culture for group A streptococcus were negative. Blood work included an elevated white blood cell count of 31,000/µL and normal liver function.
Chest radiography incidentally revealed a radio-opaque foreign body in the stomach (Figure 3). The boy then admitted to accidentally swallowing a quarter while throwing it up in the air and trying to catch it in his mouth; this occurred 1 day before the onset of the eruption.
 SYSTEMIC CONTACT DERMATITIS: AN OVERVIEW
SYSTEMIC CONTACT DERMATITIS: AN OVERVIEW
The patient’s clinical and laboratory assessment led us to the diagnosis of a systemic nickel hypersensitivity reaction, also known as systemically reactivated allergic contact dermatitis or systemic contact dermatitis (SCD) to nickel. SCD from nickel hypersensitivity is usually a type IV reaction, also known as delayed-type hypersensitivity, although cases of type I hypersensitivity to nickel have also been reported.1
SCD occurs in children and adults who typically become initially sensitized with a localized cutaneous exposure to an allergen and are subsequently systemically re-exposed to the allergen by ingestion, inhalation, or percutaneous administration.2 Body piercing, in particular ear piercing, is an important risk factor for nickel sensitization. SCD has diverse presentations, which include vesicular hand eczema and the well-demarcated redness on thighs and buttocks known as baboon syndrome. In this case, the patient’s skin eruption indicated a severe and generalized form of SCD caused by nickel ingestion. The changes seen on biopsy represented those most commonly seen after skin exposure to an allergen, resulting in a delayed–type IV hypersensitivity reaction.
NICKEL ALLERGY
Nickel allergy is the most frequently reported metal allergy. Nickel is the most common allergen in patients who undergo skin patch testing, especially in women and in teens and children younger than 18 years.3 The metal was named as the “Contact Allergen of the Year” in 2008 by the American Contact Dermatitis Society.4
Sources of exposure and sensitization to this ubiquitous element include jewelry, coins, eyeglass frames, watchbands, belt buckles, buttons, zippers, insecticides, dyes, and medical devices.5 Both eczematous and urticarial reactions of the intraoral and facial regions have been reported with nickel-containing orthodontic appliances.6
A recent Danish study suggests that regulation to limit allowable nickel release from products, such as jewelry, may substantially decrease nickel sensitization.7 In another study, trace amounts of nickel leached from braces into saliva seem to afford immunologic tolerance in some persons and suggests that the braces may be protective in future exposures, such as ear piercings.8
Nickel is also found in foods, such as chocolate, shellfish, and some legumes, nuts, and grains. Significant amounts of nickel in the diet of highly sensitized persons can provoke SCD, and reduction of dietary intake of nickel may benefit such
patients.9,10
MANAGEMENT
 Management of SCD consists of removal of the offending substance, if possible. Symptomatic treatment depends on the severity of symptoms. Mild pruritus resulting from SCD can be treated with cool compresses or oral antihistamines.2 Moderate to severe pruritus can be treated with topical corticosteroids or immunomodulators, such as tacrolimus or pimecroli-mus.2 Occasionally, the use of oral corticosteroids may be necessary.
Management of SCD consists of removal of the offending substance, if possible. Symptomatic treatment depends on the severity of symptoms. Mild pruritus resulting from SCD can be treated with cool compresses or oral antihistamines.2 Moderate to severe pruritus can be treated with topical corticosteroids or immunomodulators, such as tacrolimus or pimecroli-mus.2 Occasionally, the use of oral corticosteroids may be necessary.
In this patient, application of topical corticosteroids failed to adequately control the pruritus. Oral prednisone was then prescribed. A rapid response was noted with this treatment, with a decrease in the dermatitis and symptoms.
Endoscopy was deemed necessary because the quarter had lodged in the patient’s stomach. The diagnosis of SCD secondary to nickel, presenting as fever and rash, was confirmed when the “hard evidence,” a 1999 Canadian quarter, was endoscopically extracted (Figure 4). While US quarters have minimal amounts of nickel sandwiched between steel, Canadian quarters minted before 2001 contain 99% or more nickel.11
Subsequently, the prednisone was tapered (from 20 mg twice daily for 4 days to 20 mg daily for 2 days and finally to 10 mg for 1 day), with no complications. The patient had a complete recovery without sequelae.
1. Walsh ML, Smith VH, King CM. Type I and type IV hypersensitivity to nickel. Australas J Dermatol. 2010;51:285-286.
2. McDonald ME, Goodson S, Tolia V, Leung AK. Allergic reaction to nickel in the swallowed coins.Consultant For Pediatricians. 2005;4;176-180.
3. Lu LK, Warshaw EM, Dunnick CA. Prevention of nickel allergy: the case for regulation? Dermatol Clin. 2009;27:155-161, vi-vii.
4. Kornik R, Zug KA. Nickel. Dermatitis. 2008;19:3-8.
5. Schram SE, Warshaw EM, Laumann A. Nickel hypersensitivity: a clinical review and call to action.Int J Dermatol. 2010;49:115-125.
6. Kolokitha OE, Chatzistavrou E. Allergic reactions to nickel-containing orthodontic appliances: clinical signs and treatment alternatives. World J Orthod. 2008;9:399-406.
7. Thyssen JP, Johansen JD, Menne T, et al. Nickel allergy in Danish women before and after nickel regulation. N Engl J Med. 2009;360:2259-2260.
8. White JM, Goon AT, Jowsey IR, et al. Oral tolerance to contact allergens: a common occurrence?
A review. Contact Dermatitis. 2007;56:247-254.
9. Sharma AD. Relationship between nickel allergy and diet. Indian J Dermatol Venereol Leprol.2007;73:307-312.
10. Veien NK, Hattel T, Laurberg G. Low nickel diet: an open, prospective trial. J Am Acad Dermatol. 1993;29:1002-1007.
11. Royal Canadian Mint web site. www.mint.ca. Accessed January 11, 2012.