
Peer Reviewed
Cushing’s Disease

A 54-year-old woman was evaluated for a rising hemoglobin A1c (HbA1c) level and resistant hypertension. Blood pressure measurements on optimal doses of three antihypertensive agents and chlorthalidone averaged 180/105 mm Hg. Her HbA1c increased from 7.4% to 9.1% over a 4-month period. A review of systems revealed rounded facies, visual disturbances, and weight gain of 10 lb during the same time period. She denied taking corticosteroids.
Body mass index was 36 kg/m2; blood pressure, 186/111 mm Hg; and heart rate, 101 beats per minute. Moon facies, acanthosis nigricans, and a dorsocervical fat pad were observed (A and B). The patient had difficulty in rising from a squatting position without assistance. No striae or ecchymoses were visible, and the skin was not thinned. Visual fields by confrontation were normal.
Cushing’s syndrome was strongly suspected, and first-line screening tests for endogenous hypercortisolism were performed. The 24-hour urine free cortisol level was 171 mcg (reference range, 4 to 50 mcg/24 hours), and the 1-mg overnight dexamethasone suppression test failed to suppress the 8 AM cortisol level to less than 5 mcg/dL (patient’s 8 AM serum cortisol, 25.3 mcg/dL).
Given the markedly abnormal results of the two screening tests, the patient was referred to an endocrinologist for further work-up on the source of the endogenous hypercortisolism. Plasma adrenocorticotropic hormone (ACTH) levels on two occasions were 338 pg/mL and 464 pg/mL, respectively, which strongly indicates ACTH-dependent Cushing’s syndrome (values greater than 15 to 20 pg/mL are consistent with ACTH-dependent Cushing’s syndrome).
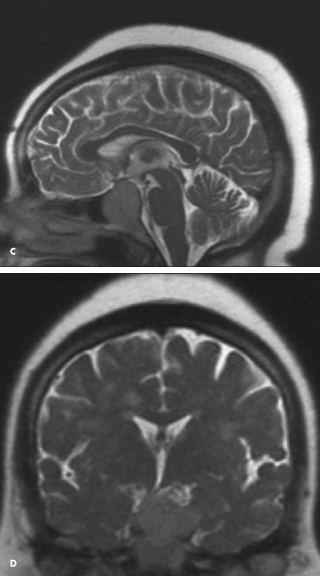
Pituitary MRI with gadolinium should be performed in all patients with ACTH-dependent Cushing’s syndrome.1,2 The patient’s MRI scan showed a 3.7 3 2.7 3 2.0 cm sellar mass with encroachment on the optic chiasm (C and D).
 Cushing’s disease due to pituitary macroadenoma is uncommon and accounts for fewer than 4% to 10% of cases. Most cases of Cushing’s disease are the result of microadenomas, particularly tumors smaller than 6 mm, which can easily be missed on imaging studies. Therefore, in cases in which the results of clinical, biochemical, and radiologic studies are discordant or equivocal, bilateral inferior petrosal sinus sampling should be performed at a center with extensive experience in this procedure.
Cushing’s disease due to pituitary macroadenoma is uncommon and accounts for fewer than 4% to 10% of cases. Most cases of Cushing’s disease are the result of microadenomas, particularly tumors smaller than 6 mm, which can easily be missed on imaging studies. Therefore, in cases in which the results of clinical, biochemical, and radiologic studies are discordant or equivocal, bilateral inferior petrosal sinus sampling should be performed at a center with extensive experience in this procedure.
This patient underwent endoscopic transsphenoidal resection of her macroadenoma with an incomplete resection of the tumor. At a postoperative office visit 45 days later her blood pressure was 140/90 mm Hg on a regimen of lisinopril 50 mg daily, amlodipine 5 mg daily, and labetalol 500 mg twice daily.
Resistant hypertension—defined as a blood pressure that remains above goal despite treatment with three antihypertensive medications of different classes, including a diuretic—is a frequently encountered problem in primary care practice.3 Determining which patients need further laboratory evaluation for secondary causes of hypertension is challenging, particularly when it comes to Cushing’s syndrome. Cushing’s syndrome due to endogenous cortisol hyperproduction is very rare, and the signs and symptoms greatly overlap with more common diseases such as diabetes, obesity, and polycystic ovarian syndrome. Because Cushing’s syndrome is potentially curable, the diagnosis should be pursued in patients whose clinical course and presentation strongly suggest endogenous hypercortisolism.n
REFERENCES:
1. Boscaro M, Arnaldi G. Approach to the patient with possible Cushing’s syndrome. J Clin Endocrinol Metab. 2009;94:3121-3131.
2. Arnaldi G, Angeli A, Atkinson AB, et al. Diagnosis and complications of Cushing’s syndrome: a consensus statement. J Clin Endocrinol Metab. 2003;88:
5593-5602.
3. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart
Association Professional Education Committee of the Council for High Blood Pressure Research.
Hypertension. 2008;51:1403-1419.
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Army or the US Government.