
Peer Reviewed
Inguinal Hernia in a 2-Year-Old Boy
AUTHORS:
Phillip Jenkins1 • Rebekah Soto, MD2 • Carlos A. Arango, MD2
AFFILIATIONS:
1Medical Student, University of Florida College of Medicine, Gainesville, Florida
2Department of Pediatrics, University of Florida College of Medicine, Gainesville, Florida
CITATION:
Jenkins P, Soto R, Arango CA. Inguinal hernia in a 2-year-old boy. Consultant. 2022;61(1):e19-e21. doi:10.25270/con.2021.04.00008
Received December 14, 2020. Accepted January 4, 2021. Published online April 14, 2021.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Carlos A. Arango, MD, Department of Pediatrics, University of Florida, 8399 Bayberry Road, Jacksonville FL, 32256 (carlos.arango@jax.ufl.edu)
A 2-year-old boy, who was adopted from Haiti as an infant, presented with his parents to our pediatrics clinic with a 3-week history of intermittent constipation and a 1-day history of emesis. The emesis had begun the morning prior to presentation while the boy was at school. Prior to the episode, the patient was more fatigued and less active than normal.
The patient was unable to keep down solid food or liquids for approximately 18 hours and had several episodes of abdominal pain. He also had bouts of constipation for approximately 3 weeks. Previous visits with his pediatrician had been via secure messaging. The pediatrician had recommended an over-the-counter laxative for the patient’s constipation.
On the day of presentation, the patient’s abdominal pain had resolved, but he was unable to tolerate oral liquids without emesis, prompting the parents to seek medical evaluation.
Physical examination. Upon arrival to our office, the patient was ill-appearing, alert, and well below his baseline activity level. The initial examination for all systems was not significant, although the patient was ill-appearing and listless. His abdomen was soft, nondistended and nontender, without appreciable masses or organomegaly.
Pathologies that can lead to vomiting in a previously healthy 2-year-old include intussusception, anatomical abnormalities such as malrotation with volvulus, toxin ingestion, functional constipation, food poisoning, bowel obstruction, and gastroesophageal reflux disease. Therefore, a thorough physical examination, including a genital examination, was performed.
The genitourinary examination revealed a 2 × 2 cm bulge in the right groin. The groin mass was tender to palpation and was not able to be easily reduced in the primary care office.
Management and treatment. The patient was taken to the emergency department where the suspected inguinal hernia was reduced after the patient received intravenous pain medication. An inguinal ultrasonography scan was performed, results of which confirmed the presence of inguinal hernias (Figures 1 and 2). The patient was admitted to the hospital with orders not to take any medications or food by mouth and was scheduled for surgery the next morning.
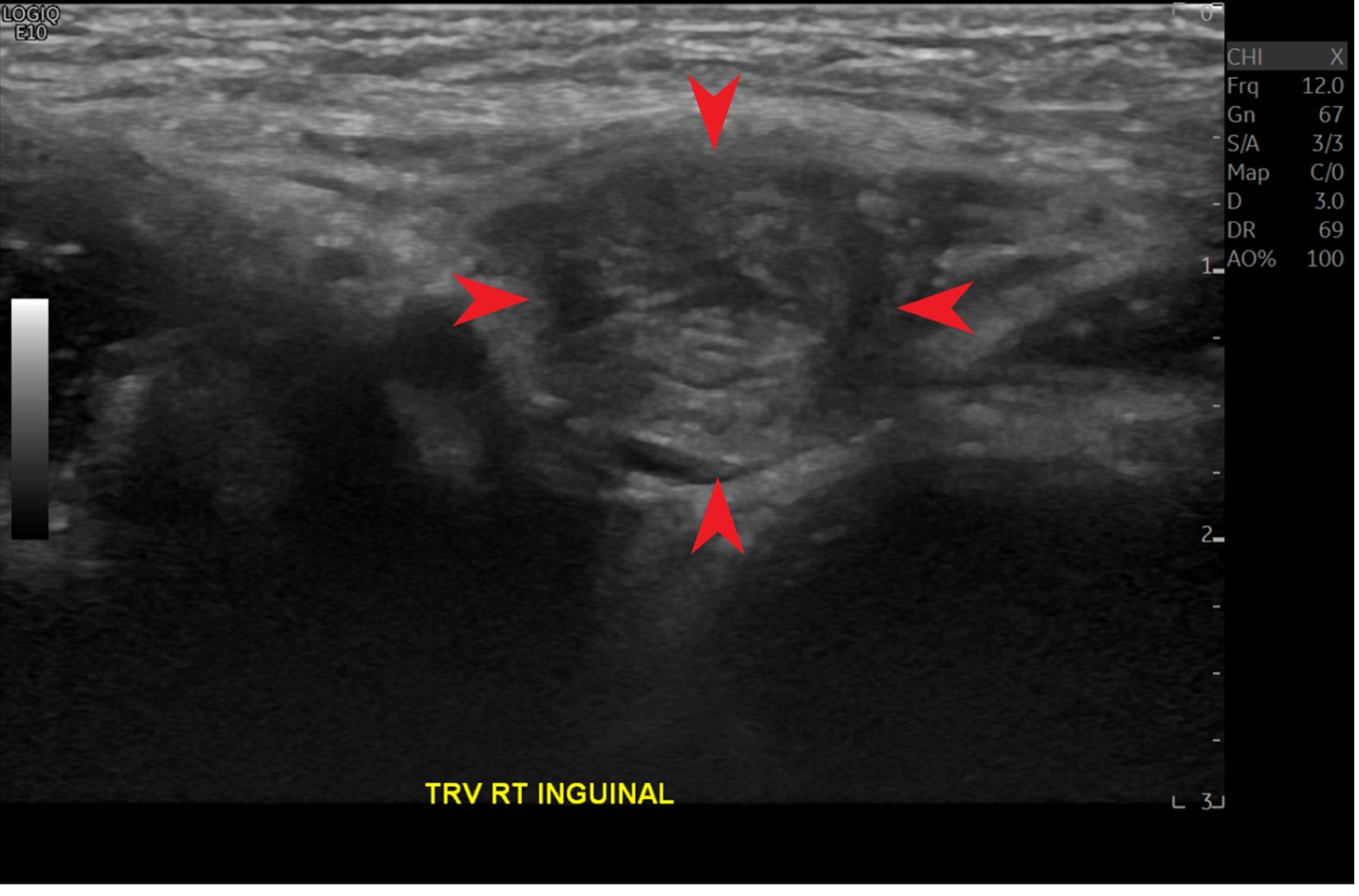
Figure 1. A right inguinal canal with hernia sac is identified (arrows).

Figure 2. A right inguinal canal with hernia sac (red arrows) and the iliac vessels (yellow arrows) are visualized. These are helpful markers when identifying inguinal hernias on the transverse view of the sonogram.
Discussion. Inguinal hernias are a common condition affecting the pediatric population.1 This condition is usually caused by an incomplete closure of the processes vaginalis and more commonly effects boys than girls at a rate of 4.27:1.2 The ratio between unilateral and bilateral hernias in both sexes is 3.77:1.2
The potential complications from an inguinal hernia include incarceration and strangulation of the bowel, which can lead to intestinal necrosis and death if untreated.3 Symptoms of an incarcerated inguinal hernia can include those of a small bowel obstruction (ie, nausea, vomiting, inability to pass stool or gas), a palpable mass, and pain in the groin. The diagnosis is usually made clinically upon physical examination when a bulge is palpated in the groin, scrotum, or labia majora and can be confirmed with ultrasonography.
The most common age of presentation of inguinal hernias is in infants younger than 1 year of age, with the majority of cases occurring in the first month of life.4 By age 2 years, the processes vaginalis usually completely closes, reducing the risk of inguinal hernias in children after this point.
Treatment for an incarcerated inguinal hernia is emergent manual reduction, followed by a hernia repair procedure to prevent recurrence.5 Bilateral inguinal hernias are rare, and routine exploration is not typically indicated for most patients, although it may be prudent if an examination or ultrasonography scan indicate bilateral hernias may be present.
Conclusions. This case highlights a few challenges that primary care pediatricians currently face. In the era of the COVID-19 pandemic, a large number of sick visits are being pushed to the telemedicine venue. There are obvious advantages to this, including reducing exposure to illness, convenience for families, and decreased costs. However, our case of a 2-year-old with a history that could be mistaken for a viral gastrointestinal illness or constipation highlights the importance of a trained pediatrician performing a physical examination to reach the correct diagnosis.
Our patient was toilet trained, so his parents were unaware of the bulge in his groin, and the boy did not report pain in the area. The parents were concerned for a gastrointestinal infectious cause or worsening constipation, and if they had opted for a telemedicine visit or continued to attempt management via secure messaging, the true diagnosis would have been delayed. The consequences of such a delay could have potentially led to bowel necrosis, perforation, and an extremely hazardous clinical course.
In a digital age, this case serves as a reminder that performing a thorough physical examination in the office is of paramount importance to reach the correct diagnosis. Because the patient was aged older than 2 years, was not concerned with pain surrounding the hernia, and was toilet trained, it made for a perfect storm to miss the diagnosis. With the history of a possible gastrointestinal infection that was obtained from school, along with concurrent functional constipation, a provider on a telemedicine visit could have easily opted to pursue conservative management of stool softeners for the constipation and antiemetics for the vomiting. This diagnosis made by physical examination could have easily been missed if the visit was not done in the office or if the physical examination was incomplete.
Patient outcome. The surgical procedure was performed with a preoperative diagnosis of incarcerated inguinal hernia and umbilical hernia. The surgeons performed a bilateral inguinal hernia repair along with an umbilical hernia repair. The patient’s postoperative course was unremarkable.
During the procedure, the surgeons discovered a left-sided hernia, as well as the known right-sided hernia. There was a 10-cm segment of small bowel with serosal injury with diffuse ecchymosis secondary to incarceration. The segment of bowel was exteriorized via the umbilical hernia and was repaired prior to being placed back into the abdomen. The umbilical hernia was subsequently repaired at closure.
References
1. Esposito C, Escolino M, Turrà F, et al. Current concepts in the management of inguinal hernia and hydrocele in pediatric patients in laparoscopic era. Semin Pediatr Surg. 2016;25(4):232-240. https://doi.org/10.1053/j.sempedsurg.2016.05.006
2. Pan ML, Chang WP, Lee HC, et al. A longitudinal cohort study of incidence rates of inguinal hernia repair in 0- to 6-year-old children. J Pediatr Surg. 2013;48(11):2327-2331. https://doi.org/10.1016/j.jpedsurg.2013.06.004
3. Zwols TLR, Akkersdijk WL, Bökkerink WJV, Andeweg CS, Pierie JPEN, Koning GG. Emergency TREPP for strangulated inguinal hernia repair: a consecutive case series. Surg J (N Y). 2020;6(2):e62-e66. https://doi.org/10.1055/s-0040-1705171
4. Aboagye J, Goldstein SD, Salazar JH, et al. Age at presentation of common pediatric surgical conditions: Reexamining dogma. J Pediatr Surg. 2014;49(6):995-999. https://doi.org/10.1016/j.jpedsurg.2014.01.039
5. Birindelli A, Sartelli M, Di Saverio S, et al. 2017 update of the WSES guidelines for emergency repair of complicated abdominal wall hernias. World J Emerg Surg. 2017;12:37. https://doi.org/10.1186/s13017-017-0149-y