
How Does Cardiometabolic Risk Present?
Pseudotumor Cerebri
Leonid Skorin, Jr., DO, MS
Fort Lea, MN
A 34-year-old woman presented with chronic headache that worsened when she bent forward and episodes of usually unilateral vision loss. The vision loss occasionally occurred in both eyes simultaneously. The patient described the events as either "grayouts" or "blackouts" from which she would completely recover in a few seconds. During the examination, she complained that her ability to drive was impaired by the frequency of these episodes.
The patient was obese; she was 50% over the ideal weight for her height. Visual acuity in both eyes was 20/20. There was no afferent pupillary defect. Color vision was normal in both eyes.
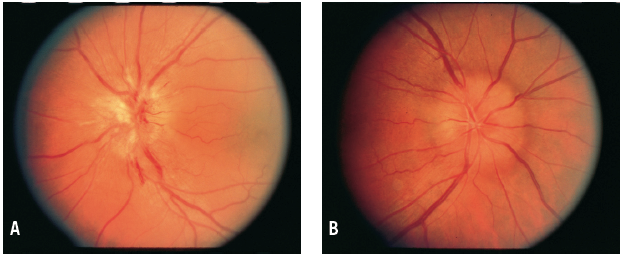
A fundus examination revealed bilateral disc edema (papilledema), more pronounced in the left eye (Figure A) than in the right eye (Figure B). Formal visual field testing found enlarged blind spots and early nasal constriction of the visual fields in both eyes. Other ophthalmic and neurologic findings were unremarkable.
An MRI scan of the brain identified no space-occupying lesion or other pathologic condition. The opening pressure during a lumbar puncture was elevated at 385 mm H2O; the cerebrospinal fluid composition was normal.
This patient had pseudotumor cerebri, which occurs primarily in obese young women. Typically, patients experience the symptoms and signs of increased intracranial pressure—including headache, transient visual obscurations, diplopia from lateral recti paresis, and photopsia, as well as nonvisual symptoms of dizziness, nausea, vomiting, tinnitus, and intracranial noises. Papilledema is the most common sign of pseudotumor cerebri.
In many patients with pseudotumor cerebri, vision improves spontaneously, although nearly half will have some vision or visual field loss, and half of these will have more serious vision impairment.
Treatment is unnecessary when visual function is normal and the patient has no symptoms. Prophylactic vascular headache remedies can be given to patients in whom headache is the only symptom. Strongly encourage weight loss for the obese patient, since loss of about 6% of total body weight can cause marked papilledema to resolve.1
Begin therapy with acetazolamide for those patients whose vision is compromised. When medical treatment fails and the threat to vision remains, surgical maneuvers—such as lumbar-peritoneal shunting or optic nerve sheath decompression—are indicated.
Reference:
1. Johnson LN, Krohel GB, Madsen RW, March GA Jr. The role of weight loss and acetazolamide in the treatment of idiopathic intracranial hypertension (pseudotumor cerebri). Ophthalmology. 1998;105(12):2313-2317.
Facial Acanthosis Nigricans
James W. Click, MD, and Barbara B. Wilson, MD
Charlottesville, VA
For the past 7 years, an obese 22-year-old African American woman presented with asymptomatic, velvety hyperpigmentation on both cheeks. Similar hyperpigmentation was present on the neck, in the axillae, and on the elbows. The patient’s only medications were antihypertensives.
Acanthosis nigricans has been linked to obesity, insulin resistance, endocrine disorders, familial inheritance, genetic variations, internal malignancies, and a plethora of drugs. This nonspecific dermatologic manifestation is characterized by symmetric velvety hyperpigmentation and typically occurs in the flexural areas of the skin, such as the axillae and neck. It may also occur on the scalp, palms, and face.1

Most cases of facial acanthosis nigricans are associated with a paraneoplastic process. Typically, acanthosis nigricans associated with a paraneoplastic process can be distinguished from other varieties by its rapid onset, extensive involvement, hyperkeratosis of the palmoplantar surfaces, and generalized pruritus.2 However, rare reports are emerging of facial acanthosis nigricans with a more gradual onset.
Most patients who have the more limited and slower-onset facial acanthosis nigricans are obese and have hyperinsulinemia; the hyperpigmentation usually develops over the temples3 and forehead.4 In one reported case, however, a non-obese child with no known endocrine abnormalities or underlying malignancy had acanthosis nigricans in the alar and melolabial folds.5
This patient had an elevated insulin C-peptide level of 10.9 ng/mL (normal range, 0.5-2.0 ng/mL) and a hemoglobin A1c level of 6.4% (normal level, less than 6%). She reported a family history of type 2 diabetes mellitus, irregular menstrual cycles, and hirsutism on the chest and face, but she denied acne and hair loss. She was further evaluated by an endocrinologist, who suspected she had type 2 diabetes, as well as polycystic ovarian syndrome. Thus, depending on the rate of onset and associated cutaneous findings, facial acanthosis nigricans should raise clinical suspicion for either an underlying malignancy or a metabolic disorder.3
Aesthetic treatment is generally ineffective, although lactic acid, topical urea, salicylic acid, calcipotriol, and retinoids have all been used with anecdotal success. Metformin6 and weight loss7 may improve the appearance of acanthosis nigricans. In one reported case, a patient with long-standing facial acanthosis nigricans, which had proved resistant to dermabrasion, tretinoin, calcipotriol, and systemic etretinate, noted aesthetic improvement after carbon dioxide laser resurfacing.8
References:
1.Katz AS, Goff DC, Feldman SR. Acanthosis nigricans in obese patients: presentations and implications for prevention of atherosclerotic vascular disease. Dermatol Online J. 2000;6(1):1.
2.Schwartz RA. Acanthosis nigricans. J Am Acad Dermatol. 1994;31(1):1-19.
3.Veysey E, Ratnavel R. Facial acanthosis nigricans associated with obesity. Clin Exp Dermatol. 2005;30(4):437-439.
4.Hisler BM, Savoy LB. Acanthosis nigricans of the forehead and fingers associated with hyperinsulinaemia. Arch Dermatol. 1987;123(11):1441-1442.
5.Akyol M, Polat M, Ozcelik S, et al. Acanthosis with atypical localization. Acta Derm Venereol. 2000;80:399.
6.Walling HW, Messingham M, Myers LM, et al. Improvement of acanthosis nigricans on isotretinoin and metformin. J Drugs Dermatol. 2003;2(6):677-681.
7.Cruz PD, Hud JA. Excess insulin binding to insulin-like growth factor receptors: proposed mechaisms for acanthosis nigricans. J Invest Dermatol. 1992;98 (6 Suppl):82S-85S.
8.Wijnberg S, Deutman HC, Steijlen PM, et al. CO2 laser treatment of benign juvenile acanthosis nigricans. Eur J Plastic Surg. 2000;23:238-240.
Acrochordons or Skin Tags
Robert P. Blereau, MD
Morgan City, LA
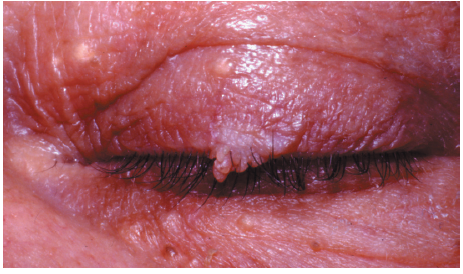
For years, a 60-year-old obese woman with type 2 diabetes mellitus had this warty lesion on the outer tarsal plate in the middle of the left upper eyelid. It was asymptomatic.
She had a few asymptomatic epidermal inclusion cysts on the upper and lower eyelids. Acrochordons, or skin tags, are associated with diabetes mellitus, dyslipidemia, acromegaly, acanthosis nigricans and, possibly, colon polyps. The most common sites are the axillae, neck, groin, and eyelids, and the skin beneath pendulous breasts.
Acrochordons are particularly common in overweight women; in autopsy series of obese women, approximately 50% were found to have skin tags.1
Treatment of acrochordons is typically for cosmesis only. Under local anestheisa, this patient’s lesion was excised in the office and its base was lightly electrocoagulated.
Reference:
1. Weedon D. Skin Pathology. 2nd ed. London: Churchill Livingstone; 2002:921.