Peer Reviewed
Can You Identify the Cause of This Patient’s Chest Pain?
Answer: Spontaneous Pneumothorax
A primary spontaneous pneumothorax occurs in a person without a known injury or event and without an underlying precipitating medical condition. Most patients who are predisposed to primary spontaneous pneumothorax have subpleural blebs that eventually rupture into the pleural cavity, causing the pneumothorax.
Primary spontaneous pneumothorax is more prevalent in men than in women and is classically seen in a tall, thin man younger than 30 years old.1 Smoking is a significant risk factor for primary spontaneous pneumothorax, with the risk of incident directly related to the patient’s smoking history. The relative risk of developing a primary spontaneous pneumothorax was found to be 7 times higher in light smokers, 21 times higher in moderate smokers, and 102 times higher in heavy smokers.2 Genetic predisposition is possible, with primary spontaneous pneumothoraxes more prevalent within certain families, but genetic testing is often completed after the event to explain the reason but not to diagnose the chest pain.
A secondary spontaneous pneumothorax develops as a complication of an underlying lung disease, most commonly chronic obstructive pulmonary disease. Persons with cystic fibrosis, lung cancer, HIV, or collagen and elastin abnormalities (eg, Marfan syndrome, Ehlers-Danlos syndrome) are also susceptible to developing a secondary spontaneous pneumothorax.
Traumatic pneumothorax is the most common and the most easily understood. These occur due to an accident that penetrates the chest wall or a medical procedure that introduces air into the pleural space.
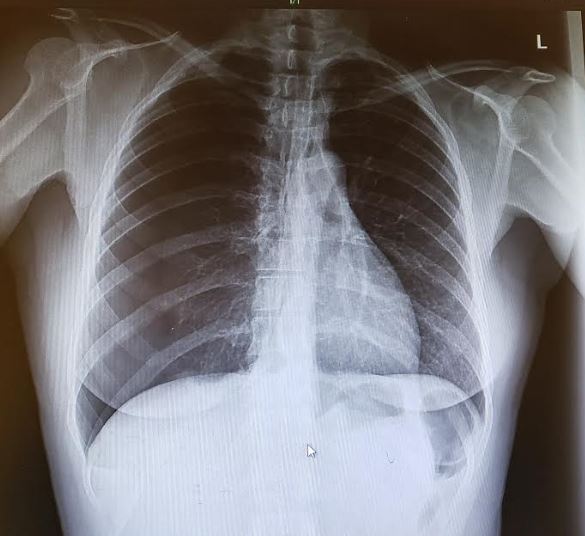
The presentation of this patient’s primary spontaneous pneumothorax was unique in that she had experienced the chest pain for 4 days, with no underlying medical condition and no smoking history. Although she was thin, she was 39 years old and female—characteristics that do not put spontaneous primary pneumothorax high on the differential diagnosis. The key to determining the diagnosis of spontaneous pneumothorax lies in the interpretation of chest radiographs. On this patient’s radiograph, the bronchovascular markings are seen clearly on the left and extend to the edge of the chest cavity. On the right side, there is a visible visceral pleural edge and no lung markings seen peripheral to the line. The radiograph shows a classic example of a right-sided pneumothorax.

Acid reflux was high on the differential due to her medical history. Because her symptoms improved with the gastrointestinal cocktail, and because her laboratory test results and ECG findings were normal, acid reflux appeared to be the most likely cause of her chest discomfort until the chest radiograph was obtained.
Costochondritis was high on the differential, as well, given the presence of what the patient described as accompanying muscle pain as well as her intense workout routine. NSTEMI was ruled out based on the normal laboratory test results and ECG findings, and rib fracture or injury was ruled out based on the chest radiograph. Angina was less likely due to normal heart rate, normal blood pressure, absence of a personal or family history of heart disease, and the prolonged 4-days presentation of chest pain.
Outcome of the case. The patient was transported from the urgent care clinic to a hospital emergency department, where she underwent chest tube insertion and was admitted to the intensive care unit.
REFERENCES:
- Melton LJ III, Hepper NG, Offord KP. Influence of height on the risk of spontaneous pneumothorax. Mayo Clin Proc. 1981;56(11):678‐682.
- Bense L, Eklund G, Wiman L-G. Smoking and the increased risk of contracting spontaneous pneumothorax. Chest. 1987;92(6):1009‐1012. doi:10.1378/chest.92.6.1009