
Peer Reviewed
Cardiac Tamponade: A Rare Presentation of Non-Small Cell Lung Cancer
Authors:
Ankit Agrawal, MD
Resident Physician, Saint Peter’s University Hospital/Rutgers Robert Wood Johnson Medical School, New Brunswick, New Jersey
Megan Ruben
Medical Student, Saint Peter’s University Hospital/Rutgers Robert Wood Johnson Medical School, New Brunswick, New Jersey
Harikrishna Bandla, MD
Resident Physician, Saint Peter’s University Hospital/Rutgers Robert Wood Johnson Medical School, New Brunswick, New Jersey
Citation:
Agrawal A, Ruben M, Bandla H. Cardiac tamponade: a rare presentation of non–small-cell lung cancer. Consultant. 2019;59(3):72-74.
A 52-year-old man presented to the emergency department (ED) with the chief concern of sudden-onset pleuritic chest pain, shortness of breath, and palpitations.
History. The man had a history of stage IV non-small cell lung cancer (NSCLC) that had been treated with radiotherapy and partial right lower lobe lung resection; brain metastasis to the right occipital lobe and left parietal lobe that had been treated with craniotomy and resection of the metastatic lesion and whole brain radiation therapy; seizure disorder after the metastasis; and coronary artery disease for which he had undergone placement of a drug-eluting stent. He had a 25 pack-year smoking history.
Physical examination. The patient’s blood pressure was 127/61 mm Hg in the right arm and 125/58 mm Hg in the left arm, heart rate was 102 beats/min, respiratory rate was 20 breaths/min, temperature was 36.6°C, and oxygen saturation was 95% on room air. A comprehensive physical examination revealed muffled S1 and S2 heart sounds.
Diagnostic tests. Laboratory test results are summarized in the Table.
Table. Laboratory Test Values | ||
Analyte (units) | Value | Reference Range |
White blood cell count (/µL) | 14,700 | 4000-11,000 |
Red blood cell count (× 106/µL) | 3.58 | 4.40-6.20 |
Hemoglobin (g/dL) | 9.2 | 13.0-17.0 |
Hematocrit (%) | 26.6 | 40.0-56.0 |
Platelet count (× 103/µL) | 315 | 150-400 |
Protein (g/dL) | 5.8 | 6.0-8.0 |
Albumin (g/dL) | 3.5 | 3.5-5.0 |
Urea nitrogen (mg/dL) | 10 | 6-20 |
Creatinine (mg/dL) | 0.58 | 0.66-1.25 |
Calcium (mg/dL) | 8.5 | 8.4-10.0 |
Glucose (mg/dL) | 93 | 74-106 |
Sodium (mEq/L) | 138 | 136-145 |
Potassium (mEq/L) | 3.1 | 3.5-5.1 |
Chloride (mEq/L) | 103 | 99-112 |
Bicarbonate (mEq/L) | 26 | 21-33 |
Anion gap | 9 | 8-12 |
Alkaline phosphatase (U/L) | 130 | 56-119 |
Aspartate aminotransferase (U/L) | 10 | 17-59 |
Alanine aminotransferase (U/L) | 14 | 21-72 |
Total bilirubin (mg/dL) | 0.3 | 0.1-1.2 |
Magnesium (mEq/L) | 1.3 | 1.3-2.2 |
Troponin I (ng/mL) | 0.06, 0.07 | 0-0.4 |
An electrocardiogram (ECG) revealed sinus tachycardia with nonspecific ST and T wave changes (Figure 1).

Figure 1. ECG showing sinus tachycardia.
NEXT: Diagnostic Tests (Continued)
The patient’s history of cancer and associated high suspicion for pulmonary embolism prompted computed tomography (CT) pulmonary angiography, the results of which revealed an acute right upper lobe segmental pulmonary embolus (Figure 2). A small to moderate sized pericardial effusion was also noted (Figure 3).
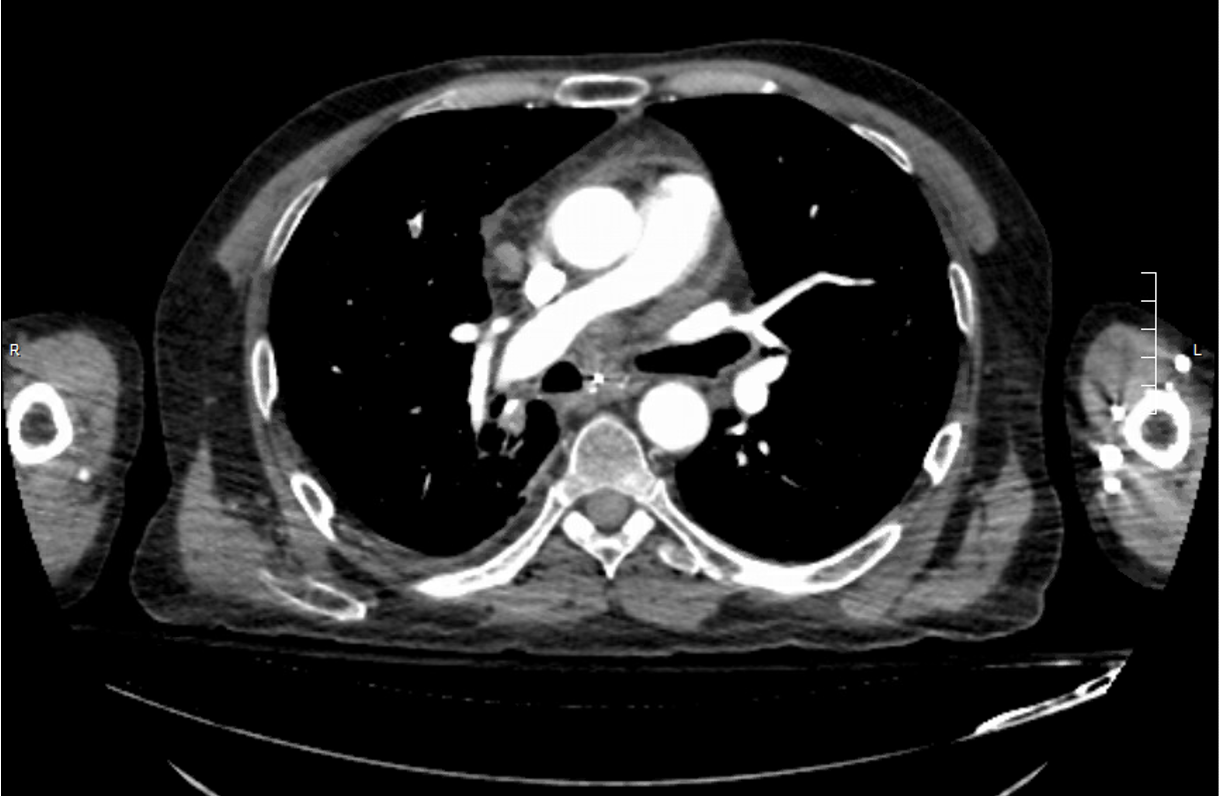
Figure 2. CT pulmonary angiography showing a small filling defect.

Figure 3. CT pulmonary angiography showing moderate sized pericardial effusion.
The patient was started on a therapeutic regimen of subcutaneous enoxaparin, 1 mg/kg twice daily, as treatment for the pulmonary embolism. He was comfortable the night of admission. The next morning, however, he reported worsening chest pain. Blood pressure at this time was 90/55 mm Hg in the right arm and 87/57 mm Hg in the left arm. Prominent jugular venous distension and muffled heart sounds were noted.
A preliminary bedside diagnosis of cardiac tamponade was made and was confirmed by urgent echocardiography, the results of which showed a large, hemodynamically significant pericardial effusion with right ventricular diastolic collapse (Figure 4).

Figure 4. Echocardiography showing a large pericardial effusion.
Hospital course. The patient was given intravenous fluid boluses, which led to hemodynamic improvement. He immediately underwent CT-guided pericardial drainage, during which 300 mL of dark bloody fluid was aspirated and a pericardial drain was left in place. He reported significant improvement in the chest pain after the procedure. Subsequent analysis of the pericardial fluid demonstrated the presence of metastatic adenocarcinoma.
Given high concern for a recurrent pericardial effusion, the patient underwent formation of a pericardial window with pericardial biopsy, the results of which again showed metastatic adenocarcinoma.
Outcome of the case. The patient had no postoperative complications and was stable at follow-up, with minimal recurrence of pericardial effusion.
NEXT: Discussion
Discussion. The pericardium is a fibroelastic sac that covers the heart. It has a parietal and visceral component, and the space between them—the pericardial space—normally contains a thin layer of less than 50 mL of an ultrafiltrate of plasma called pericardial fluid. Cardiac tamponade is a pericardial compressive syndrome resulting from an accumulation of pericardial fluid under pressure. It is a life-threatening emergency. It can present acutely, subacutely, or be occult. Malignancy-related pericardial effusion resulting in tamponade is subacute and is most commonly from cardiac metastases (eg, lung cancer, breast cancer, lymphoma) rather than primary cardiac tumors. Dyspnea is the most common symptom of cardiac tamponade and sometimes can be a presenting sign of the neoplasm.1
Cardiac tamponade is classically characterized by the Beck triad: hypotension, dilated neck veins, and muffled heart sounds.2 Tachycardia and pulsus paradoxus are other notable physical examination findings. As a part of diagnostic workup, chest radiography reveals an enlarged cardiac silhouette,3 and ECG usually shows a low-voltage waveform and electrical alternans.4 Low QRS voltage usually resolves 1 week after pericardiocentesis.5 Troponin I and creatinine kinase levels can be elevated but do not carry any prognostic value.6
Collapse of the right atrium at end diastole and the right ventricle in early diastole are hallmark findings on echocardiography and reflect intrapericardial pressure exceeding intracardiac pressure during diastole.3 Echocardiography is an extremely important diagnostic tool, since it can detect pericardial effusion even before overt tamponade.7 Our patient had evidence of right ventricular diastolic collapse (Figure 3), which is a less sensitive but more specific finding of tamponade.
Acute tamponade is usually caused by trauma or cardiac rupture or as a complication of diagnostic or therapeutic procedures such as cardiac catheterization. Subacute tamponade more commonly results from neoplasm or idiopathic pericarditis. Malignancy accounts for 32% of cardiac tamponade cases,8 the most common of which is lung cancer, with NSCLC accounting for 5% of cases.
Catheter drainage is the most common initial treatment approach. An indwelling catheter commonly is left in place until the drainage is less than 20 to 30 mL/day. Surgical decompression, with formation of a pericardial window, may be performed when there is a higher probability of pericardial effusion recurrence to allow drainage of fluid into the pleural or peritoneal cavity. Recurrent malignant effusion can exceed 90%10 and is a poor prognostic indicator. For these patients, the primary goal should be symptomatic treatment directed at improving quality of life.9
References:
- Burazor I, Imazio M, Markel G, Adler Y. Malignant pericardial effusion. Cardiology. 2013;124(4):224-232.
- Beck CS. Two cardiac compression triads. JAMA. 1935;104(9):714-716.
- Adler Y, Charron P, Imazio M, et al; ESC Scientific Document Group. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015;36(42):2921-2964.
- Bruch C, Schmermund A, Dagres N, et al. Changes in QRS voltage in cardiac tamponade and pericardial effusion: reversibility after pericardiocentesis and after anti-inflammatory drug treatment. J Am Coll Cardiol. 2001;38(1):219-226.
- Sánchez-Enrique C, Nuñez-Gil IJ, Viana-Tejedor A, et al. Cause and long-term outcome of cardiac tamponade. Am J Cardiol. 2016;117(4):664-669.
- Decamp MM Jr, Mentzer SJ, Swanson SJ, Sugarbaker DJ. Malignant effusive disease of the pleura and pericardium. Chest. 1997;112(suppl 4):291S-295S.
- Oliver C, Marín F, Pineda J, et al. Low QRS voltage in cardiac tamponade: a study of 70 cases. Int J Cardiol. 2002;83(1):91-92.
- Imazio M, Brucato A, Barbieri A, et al. Good prognosis for pericarditis with and without myocardial involvement: results from a multicenter, prospective cohort study. Circulation. 2013;128(1):42-49.
- Petrofsky M. Management of malignant pericardial effusion. J Adv Pract Oncol. 2014;5(4):281-28
- Refaat MM, Katz WE. Neoplastic pericardial effusion. Clin Cardiol. 2011;34(10):593-598.