
Allergic Rhinitis: Nothing to Sneeze at
 What is the impact of allergic rhinitis on medical costs and patients’ quality of life?
What is the impact of allergic rhinitis on medical costs and patients’ quality of life?
What primary care disease is “ignored, underdiagnosed, misdiagnosed, and mistreated, which not only is detrimental to health, but also has societal costs”?1 A recent “Top Paper”1 makes a strong case that it is allergic rhinitis. The entity can be defined as an inflammatory disorder of the nasal mucosa with pruritus, sneezing, rhinorrhea, and nasal congestion mediated by early- and late-phase hypersensitivity responses. Allergic rhinitis is increasing in prevalence throughout primary care practices. Let’s look at the cautionary words in the introductory sentence—as a precautionary “did you know” (I didn’t)—from this important paper.
_________________________________________________________________________________________________________________________
RELATED CONTENT
Allergic Contact Dermatitis From Tea Tree Oil
Allergic Rhinitis and Asthma: How to Help Patients
_________________________________________________________________________________________________________________________
“SOCIETAL COST”
•Children in the United States miss approximately 2 million school days a year because of allergic rhinitis.
•Performance on school examinations by adolescents 15 to 16 years of age in the United Kingdom is worsened by allergic rhinitis, especially if the adolescents are taking antihistamines that cause sedation.
•These statistics add up: perennial allergic rhinitis impairs health-related quality of life as much as asthma does.
“DETRIMENTAL TO HEALTH”
•Children with allergic rhinitis who are exposed to their inciting antigen and who then acquire a simultaneous “cold” have an odds ratio of 19 for an asthma hospital admission.
•Children with allergic rhinitis have more intense viral colds.
•There is a higher prevalence of asthma among persons who have allergic rhinitis.
“IGNORED, UNDERDIAGNOSED, AND MISDIAGNOSED”
•Four hundred million people worldwide have allergic rhinitis.
•A high index of suspicion is required for diagnosis. Consider the diagnosis in patients with symptoms of nasal itching, sneezing, nasal obstruction or congestion, rhinorrhea, and occasionally a reduction in smell.
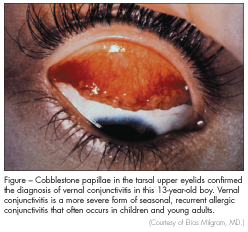
•Fifty to seventy percent of persons with allergic rhinitis have allergic conjunctivitis (Figure).
•Specific IgE reactivity to airborne allergens is required to diagnose this disease (the allergist as consultant).
“MISTREATED”
•Intranasal corticosteroids are the most effective therapeutic agents for allergic rhinitis.
•Two pharmacological treatments are not advised. Antihistamines that cause sedation worsen academic and work performance, and they also increase the likelihood of auto and industrial accidents. Intramuscular corticosteroid injections can cause untoward systemic effects and subcutaneous and muscular necrosis.
MORE THAN JUST A NUISANCE
The article contains helpful diagnostic and therapeutic algorithms.1 I am guilty. I have had a bad habit of viewing allergic rhinitis as a nuisance. The data in the “Top Paper” reminded me it is a serious disease that demands more primary care respect.
1. Greiner AN, Hellings PW, Rotiroti G, Scadding GK. Allergic rhinitis. Lancet. 2012;378:2112-2122.