
17-Year-Old Girl with Painful Toe Swelling

HISTORY
A 17-year-old Canadian girl complains of painful swelling on all her toes, which started 10 days earlier when the weather was very cold. She used to walk around barefoot in a poorly insulated basement.
The pain is worse with sweating and on days when the weather is cold. There is no associated fever, joint symptoms, or weight loss. Her past health is unremarkable. In particular, she has no history of Raynaud phenomenon or collagen vascular disease. She does not smoke. All other family members are healthy.
PHYSICAL EXAMINATION
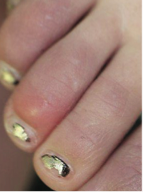
Vital signs are normal. The toes are swollen, tender, and discolored. The rest of the examination results are unremarkable.
WHAT’S YOUR DIAGNOSIS?
(Answer on next page)
Pernio (chilblains) is a localized inflammatory skin lesion that occurs after prolonged exposure of non-adapted tissue to cold, above-freezing temperatures.1,2 The condition is characterized by painful or itchy, erythematous or violaceous skin lesions; the distal extremities are most often affected.3
 EPIDEMIOLOGY
EPIDEMIOLOGY
The peak incidence is between 15 and 30 years of age, although persons in any age group can be affected.4,5 There is a female predominance.4,5 The most common trigger is exposure to cold, damp, and nonfreezing conditions.2 Pernio occurs more commonly in persons who wear cold, wet shoes or boots or who walk barefoot, especially during the winter.
PATHOGENESIS
The exact pathogenesis is not known. The condition is thought to have a vascular origin.2 Pernio has been reported in association with the presence of cryoproteins, anticardiolipin, antiphospholipids, and lupus anticoagulant; systemic lupus erythematosus; and rheumatoid arthritis.4,5
CLINICAL MANIFESTATIONS
Pernio usually develops 12 to 24 hours after exposure to the cold.4,5 Characteristically, pernio presents as symmetric, erythematous to violaceous, edematous macules, papules, nodules, or plaques.1,2 In severe cases, vesicles, bullae, and ulcers may be seen.1,2 Toes and fingers are the sites of predilection, although ears, nose, heels, and thighs may also be affected.3 Typically, patients describe itching, burning, or intense pain in the affected area.3,5
HISTOPATHOLOGY
Characteristic histologic features are dense T-cell infiltrate in the superficial and deep dermal vasculatures, dermal edema, and necrotic keratinocytes.1,3 Fibrinoid lesions can be seen in the blood vessel walls.3
DIAGNOSIS
The diagnosis is mainly clinical, based on a history of exposure to cold and the characteristic clinical features.
DIFFERENTIAL DIAGNOSIS
Frostbite occurs after exposure to extreme cold and is caused by direct ice crystal formation at the cellular level with resultant tissue necrosis.5,6 Erythema, edema, and blister formation characterize the typical lesions of superficial frostbite. Tissue necrosis, gangrene, and tissue loss can occur in deep frostbite.
Other differential diagnoses include cellulitis, contact dermatitis, Raynaud phenomenon, acrocyanosis, snake bite, spider bite, methemoglobinemia, chilblain lupus, embolic phenomenon, and peripheral vascular disease.1,4 The distinctive features of each condition allow a straightforward differentiation from pernio.
MANAGEMENT
Because of the high rate of spontaneous recovery, most patients do not require pharmacological treatment. A “watch-and-wait” approach is often recommended. Patients should be advised to avoid exposure to cold temperature and to keep the extremities warm and dry. For patients who actively desire treatment, calcium channel blockers (in particular, nifedi-pine) are the treatment of choice.3-5 The efficacy of topical fluorinated corticosteroids in the treatment of pernio is controversial.5,7,8
This patient was advised to use polypropylene socks to wick sweat away and to keep the feet warm and dry. The painful swelling of the toes subsided in 2 weeks.
PROGNOSIS
The condition is often self-limiting, lasting 1 to 3 weeks in healthy persons.1,2 Pernio may recur upon exposure to cold.
1. Brown PJ, Zirwas MJ, English JC III. The purple digit: an algorithmic approach to diagnosis. Am J Clin Dermatol. 2010;11:103-116.
2. Smith M. Environmental and sports-related skin diseases. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. Philadelphia: Mosby; 2003:1385-1410.
3. Chan Y, Tang WY, Lam WY, et al. A cluster of chilblains in Hong Kong. Hong Kong Med J. 2008;14:185-191.
4. Parra SL, Wisco OJ. What is your diagnosis? Perniosis (chilblain). Cutis. 2009;84:27-29.
5. Simon TD, Soep JB, Hollister JG. Pernio in pediatrics. Pediatrics. 2005;116:e472-e475.
6. Jurkovich GJ. Environmental cold-induced injury. Surg Clin North Am. 2007;87:247-267.
7. Burry JN. Adverse effects of topical fluorinated corticosteroid agents on chilblains. Med J Aust. 1987;146:451-452.
8. Ganor S. Corticosteroid therapy for pernio. J Am Acad Dermatol. 1983;8:136.