
Peer Reviewed
Unilateral Submandibular Lymphadenopathy in a 7-Year-Old Boy
AFFILIATIONS:
1Department of Pediatrics, McGovern Medical School at the University of Texas Health Science Center at Houston, Houston, TX
2Medical Student, McGovern Medical School at the University of Texas Health Science Center at Houston, Houston, TX
CITATION:
Beaudoin E, Mehta M, Valek S. Unilateral submandibular lymphadenopathy in a 7-year-old boy. Consultant. 2022;62(11):e6. doi:10.25270/con.2022.06.00004
Received October 3, 2021. Accepted October 25, 2021. Published online June 2022.
DISCLOSURES:
The authors report no relevant financial relationships. The authors report that informed patient consent was obtained for publication of the images used herein.
CORRESPONDENCE:
Ebony Beaudoin, MD, McGovern Medical School, 6410 Fannin Street, Suite 500, Houston, TX 77030 (ebony.williams@uth.tmc.edu)
ABSTRACT:
A 7-year-old boy presented with a 3-week history of an ulcerated vesicle on his left cheek, left-sided facial swelling, and left submandibular lymphadenopathy after being scratched by a kitten. The swelling worsened despite a course of cephalexin for an assumed case of lymphangitis. Given his history of contact with a cat and clinical presentation, he was given a presumptive diagnosis of Cat-scratch disease. He was prescribed a 5-day course of azithromycin and had full resolution of his symptoms approximately 2 weeks later. Cat-scratch disease, a bacterial infection caused by Bartonella henselae, is a common pediatric condition characterized by local lymphadenopathy and fever after being scratched by a cat. It can be diagnosed clinically based on history and physical exam findings and is usually a benign and self-limited condition in immunocompetent pediatric patients.
Keywords: Cat-scratch disease, bacterial infection, pediatrics
Cat-scratch disease is a bacterial infection caused by Bartonella henselae that most commonly presents with fever and subacute regional lymphadenopathy after being scratched by a domestic or feral cat.1 It is considered to be one of the most common causes of subacute or chronic lymphadenopathy in children, and should be considered in any pediatric patient presenting with lymphadenopathy or fever of unknown origin.2We present a case of a 7-year-old boy with a facial cutaneous lesion and submandibular lymphadenopathy after being scratched by a cat, presumptively diagnosed with Cat Scratch Disease.
Case Presentation
A 7-year-old boy presented to the outpatient pediatric clinic with a 1-week history of left-sided facial swelling (Figures 1-4).



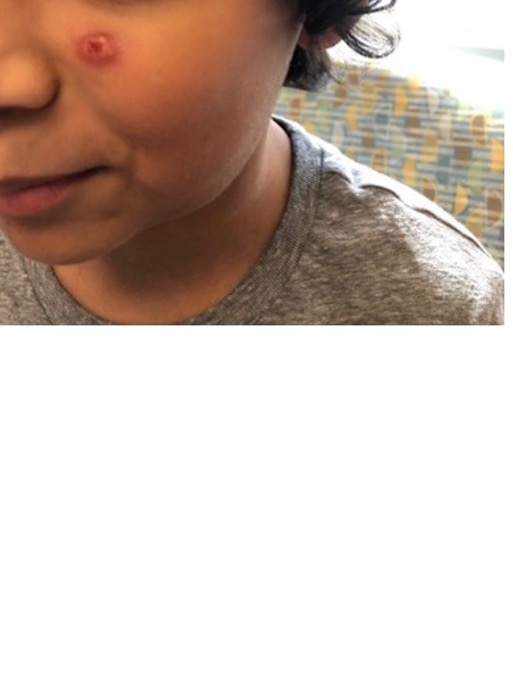
Figures 1-4. Patient on initial presentation, showing a firm erythematous nodule with an overlying vesicle and submandibular lymphadenopathy.
History. The patient had no significant past medical history. Three weeks prior, he presented to a local urgent care clinic with a vesicle on his left cheek and slightly swollen submandibular lymph node after being scratched by a kitten. His condition was diagnosed as lymphadenitis, and he was prescribed cephalexin. At the time, the lymphadenitis was attributed to recent filling of dental caries. Despite completing a 10-day course of cephalexin, he began to develop increased left-sided facial swelling without associated tenderness or erythema. The swollen area continued to enlarge over the next week. The patient had no associated symptoms of fever, eye discharge or redness, congestion, fatigue, sore throat, or change in appetite or activity. His mother denied prior history of lymphadenopathy or any change in color or drainage.
Physical examination. The patient was afebrile, alert, active, and in no acute distress. Examination of the skin revealed a 1-cm raised, firm, nontender, erythematous circular nodule adjacent to the nose on the left cheek with an overlying 3 mm to 4 mm vesicle. The vesicle was open, circular, and appeared to be healing well without exudate. The left submandibular area was swollen, painless to palpation, nonerythematous and nonfluctuant. The patient had mildly boggy nasal turbinates with no discharge. Physical examination was otherwise unremarkable.
Laboratory testing. A blood culture was drawn and showed no growth. A complete blood cell count and differential were within normal limits, with no leukocytosis.
Discussion
Cat-scratch disease is a bacterial infection caused by Bartonella henselae and most commonly presents with fever and subacute regional lymphadenopathy after an individual is scratched by a domestic or feral cat.1 Primary cutaneous lesions (typically a papule, vesicle, or nodule, as seen in our patient) usually appear 7 to 12 days after contact with a cat. Lesions may persist for 1 to 3 weeks, while lymph node enlargement and overlying erythema can take several months to resolve completely.1,2 Lymphadenopathy affects the lymph nodes draining the site of the cat scratch and is local in 85% to 90% of patients.3 While local cervical, axillary, or inguinal lymphadenopathy is most common, more diffuse lymphadenopathy can also be seen in some patients.3 Rarely, systemic manifestations of cat-scratch disease may occur such as hepatosplenomegaly, encephalitis, neuroretinitis, or bacillary angiomatosis, especially in immunocompromised patients.4 The most common atypical manifestation is ocular disease (retinitis or conjunctivitis), followed by hepatosplenic disease.4
Previous literature suggests that both typical and atypical cat-scratch disease are reported with the highest incidences in the southern United States during late summer and fall,4 both consistent with our patient’s case. The differential for unilateral lymphadenopathy includes other infectious causes, such as cytomegalovirus, Epstein-Barr virus, group A streptococcus, HIV, and toxoplasmosis, as well as malignancy, especially leukemia in children.3
Because cat-scratch disease is one of the most common causes of subacute or chronic lymphadenopathy in children, it should be considered in any pediatric patient with lymphadenopathy or fever of unknown origin.2 Prognosis for most children with cat-scratch disease is excellent, with eventual spontaneous resolution in 90% to 95% of children.1 A small minority of patients may require surgical drainage for persistent abscesses or removal of enlarged lymph nodes. Surgical intervention typically involves excisional lymphadenectomy, which is better tolerated in pediatric patients compared with fine needle aspiration or incision and drainage.5
Treatment. The clinical management of cat-scratch disease is variable among clinicians. Diagnosis is made clinically and can be confirmed via serologic testing. Gram staining is usually insensitive for B henselae and is difficult to identify by culture, as was the case with our patient with negative blood cultures. For mild to moderate cases of cat-scratch disease, treatment is not necessary, and lymphadenopathy should resolve spontaneously over 4 to 8 weeks.6 Although there is limited evidence, antibiotic treatment with azithromycin may reduce the duration of lymphadenopathy in cat-scratch disease.3 Considering our patient’s impressive lymphadenopathy, the potential clinical benefit and relatively simple course of azithromycin outweighed any potential disadvantages.
Patient outcome. Given his presentation and known history of cat contact, the patient's condition was presumptively diagnosed as cat-scratch disease. The patient was started on a 5-day course of azithromycin. Bartonella titers were ordered but never completed. The patient’s mother reported complete resolution approximately 2 weeks after initiation of azithromycin therapy. The patient did not develop any new symptoms or experience adverse effects of the antibiotic treatment.
Conclusion
Cat-scratch disease is a common condition among pediatric and adolescent patients that presents clinically with regional unilateral lymphadenopathy and fever. It should be considered in any pediatric patient with acute, subacute, or chronic lymphadenopathy, especially with a history of exposure to cats.1 Although it is usually a benign and self-limited condition in immunocompetent patients, it is an important clinical diagnosis to recognize as the differential includes more serious conditions such as cytomegalovirus, Epstein-Barr virus, group A streptococcus, HIV, toxoplasmosis, and malignancy such as leukemia.3 A thorough patient history and physical exam are critical in diagnosis and prognosis is generally excellent in immunocompetent pediatric patients.1
2. English R. Cat-scratch disease. Pediatr Rev. 2006;27(4):123-128. doi:10.1542/pir.27.4.123
3. Klotz SA, Ianas V, Elliot SP. Cat-scratch disease. Am Fam Physician. 2011;15;83(2):152-155.
4. Nawrocki CC, Max RJ, Marzec NS, Nelson CA. Atypical manifestations of cat-scratch disease, United States, 2005-2014. Emerg Infect Dis. 2020;26(7):1438-1446. doi:10.3201/eid2607.200034
5. Munson PD, Boyce TG, Salomao DR, Orvidas LJ. Cat-scratch disease of the head and neck in a pediatric population: surgical indications and outcomes. Otolaryngol Head Neck Surg. 2008;139(3):358-363. doi:10.1016/j.otohns.2008.06.030
6. Zangwill KM. Cat scratch disease and bartonellaceae: the known, the unknown and the curious. Pediatr Infect Dis J. 2021;40(5S):S11-S15. doi:10.1097/INF.0000000000002776