
Peer Reviewed
Surgical Outcome of a Perforated Gastric Carcinoma With Signet Features
AFFILIATIONS:
1Windsor University School of Medicine, Cayon, Saint Kitts and Nevis
2The Department Surgery, West Surburban Medical Center, Oak Park, IL
3Chairman, The Department of Surgery, West Suburban Medical Center, Oak Park, IL
CITATION:
Farah I, Zaarab M, Jorge JM, Tiesenga FM. Surgical outcome of a perforated gastric carcinoma with signet features. Consultant. 203;63(4):e9. doi:10.25270/con.2023.02.000001
Received August 19, 2022. Accepted November 23, 2022. Published online January 30, 2023.
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS
None.
CORRESPONDENCE:
Ibrahim Farah, MD, 503 Ponthieu Circle, Ottawa, Ontario, K1W 0N5, Canada (Ibrahim.farah11@gmail.com)
Introduction. A 51-year-old Black man presented to the emergency department (ED) with a 1-month history of abdominal pain, nausea, and non-bloody/non-bilious vomiting, which was associated with difficulty swallowing, decreased oral intake, and a weight loss of 40 pounds in the interim.
History. His past medical history was unremarkable, except daily inhalational heroin use prior to admission and a 20 pack-years smoking history. The patient underwent a splenectomy 23 years prior to presentation.
Diagnostic testing. Physical examination was remarkable for generalized abdominal tenderness and a fever of 99.8°F. Initial investigations included a complete blood count (CBC), which was notable for anemia with a hemoglobin of 6.8 g/dL. He was transfused two units of packed red blood cells. A computed tomography (CT) scan of the abdomen and pelvis without contrast showed an extraluminal air-fluid collection along the proximal lesser curvature (Figures 1 & 2).
![]()
![]()
Figures 1 & 2. Non-contrast CT of abdomen & pelvis.
Next, we ordered a CT with contrast, which showed a rim-enhancing collection extending from the gastric body. This was suspicious for a large subacute perforated gastric ulcer and a contained gastric abscess.
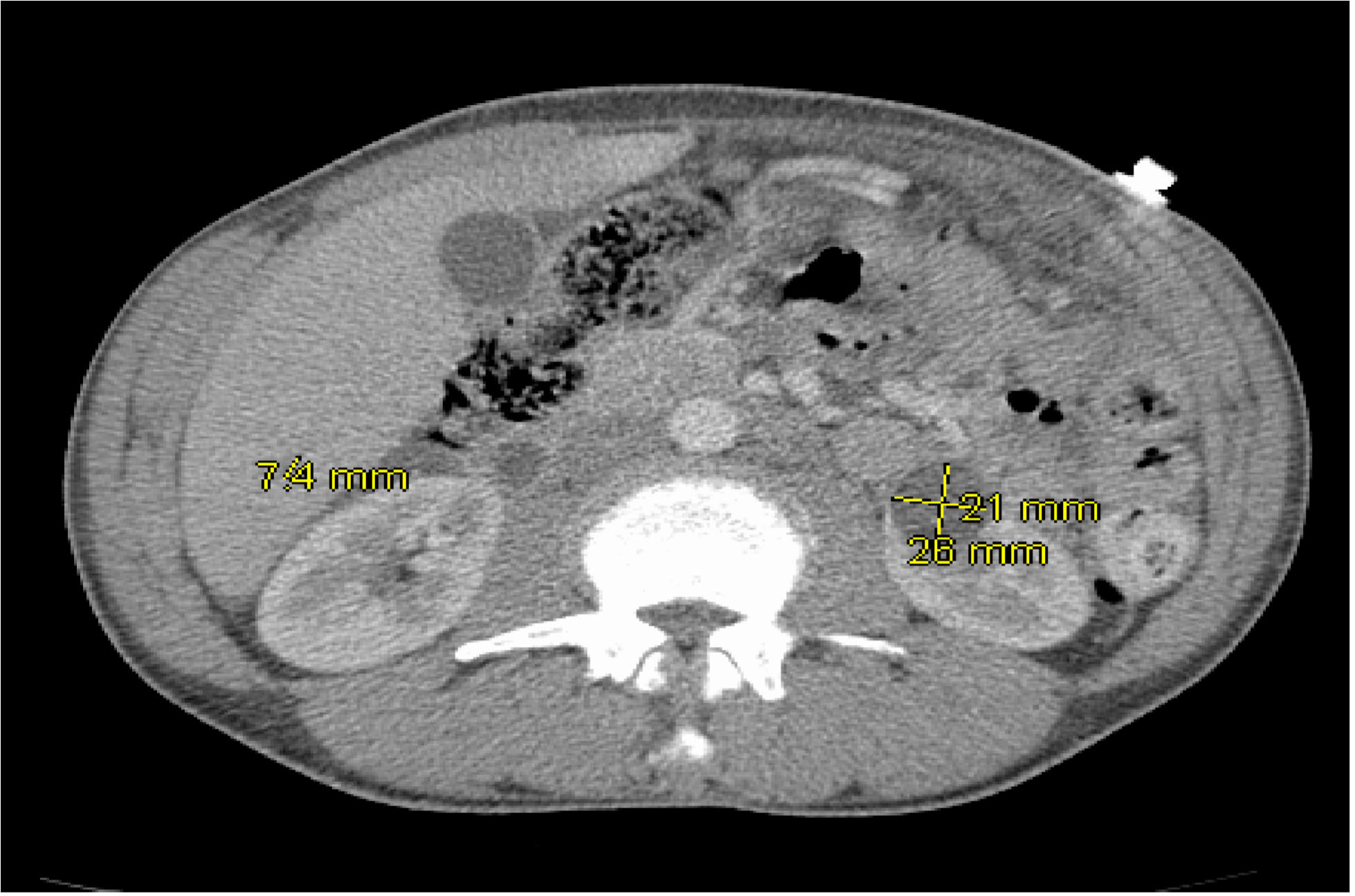
Figure 3. CT of abdomen & pelvis with contrast.
A esophagogastroduodenoscopy (EGD) was performed subsequently, which showed candida esophagitis and two large gastric ulcers arising from the lesser curvature and the antrum of the stomach (Figures 4 & 5). Additionally, a gastric biopsy from the ulcers showed a poorly differentiated adenocarcinoma with signet features and HER2/neu negative.
![]()
Figure 4. Distal body/antral stomach ulcer
![]()
Figure 5. Candida esophagitis in the esophagus.
Treatment and management. After consulting with oncology specialists, non-adjuvant chemotherapy followed by surgery was planned. A jejunostomy tube was placed for feeding along with a perma catheter for chemotherapy as an outpatient. The patient was also given ampicillin/sulbactam (1.5g/100ml intravenously every 6 hours), fluconazole (200mg orally daily), and pantoprazole (40mg intravenously twice per day) for treatment of the abscess, candida esophagitis, and stomach ulcer for a duration of 27 days.
One week later, the patient presented to the hospital again with diffuse, sharp abdominal pain. The patient was peritonitic, had a fever of 103.6º F, an elevated white blood cell (WBC) count of 18.2K/uL, and ascites on CT imaging. He was taken to the operating room for an exploratory laparotomy, during which 2L of fluid were suctioned prior to discovering he had a gastric perforation in the lesser curvature of his stomach.
Because of to the chronic nature of the abscess and its location within 5 cm of the gastroesophageal junction, the decision was made to undergo a total gastrectomy with Roux-en-Y esophagojejunostomy. The prior jejunostomy feeding tube was removed and the patient remained hemodynamically stable after surgery. His recovery was prompt due to his ability to ambulate by postoperative day 2.
![]()
Figure 6. Resected section of the stomach with perforation of gastric tumor cells.
The resected stomach was sent to pathology, revealing a high-grade mucinous carcinoma with poorly differentiated signet ring cells invading the muscularis propria into the subserosal adipose tissue, establishing it as the cause of the perforation (Figures 7-10).
![]()
Figure 7. Signet ring cells and ulcerated surface epithelium.
![]()
Figure 8. Surface epithelial ulceration.
![]()
Figure 9. Cluster of signet ring cells within lamina propria.
![]()
Figure 10. Cytokeratin stain AE1/AE3 and preserved surface epithelium.
The pathological staging of the tumor was T3N1M0, which is rare given the aggressive nature of the cancer and its high tendency to metastasize and invade adjacent structures.
Given the general condition of severe and diffuse peritonitis in our patient at time of presentation, an argument could have been made to pursue palliative therapy and perform a simple closure with an omental patch or even a subtotal gastrectomy. The results of a metanalysis study showed that postoperative complications, hospital mortality rate, and 5-year survival rate were similar in both total gastrectomy and subtotal gastrectomy patients.1 However, the aggressive and infiltrative nature of gastric signet-ring cell carcinoma (SRCC), requiring frequent resections over time, makes a good argument in opting for a total gastrectomy in this scenario.2 The diagnosis of SRCC was not made until after curative resection was completed, which gave the patient the best outcome possible in this case.
Outcome and follow-up. Our patient was 51 years old and had no comorbidities at time of presentation, which placed him in a lower risk group despite his tumor’s histopathological stage (T3N1M0). His ability to ambulate and remain hemodynamically stable and complication-free post-operatively is a good indicator for a positive long-term outcome in managing his cancer.
Discussion. SRCC is a rare and unfavorable type of malignant adenocarcinoma that has an aggressive nature and a poor prognosis. Malignant perforation is more common in advanced cases where serosal and lymph node invasion is present and the diagnosis is often made only on post-operative pathologic examination.3
A histopathological analysis is needed to confirm the presence of poorly differentiated adenocarcinoma with signet ring cell.4 These large tumor cells contain large mucin-filled vacuoles, which push the nuclei of the cells to the periphery. Early diagnosis followed by gastrectomy, regional lymphadenectomy, and postoperative chemotherapy remain the gold standard and allow for a better prognosis.
Perforation due to gastric cancer is a very rare type of complication, occurring in less than 1% of gastric cancer cases.3 The cause of perforation is not usually attributed to gastric carcinoma in the early stages, and rarely prior to emergency laparotomy.4Differentials for perforation include peptic ulcers, which are the main cause of gastric perforations and account for about 10-16% of cases of gastric cancer, and MALT lymphoma.4Risk factors for gastric perforation are similar to those of ulceration and include smoking, nonsteroidal anti-inflammatory drug use, steroid use, stress, and recent surgery.5
Perforated gastric cancer (PGC) is a severe complication, carrying a mortality rate of 8-82%.5 Studies have shown that patients who underwent curative resection for PGC had higher post-operative and long-term survival rates than patients who underwent simple closure with omental patch.5,6
When comparing SRCC and non-SRCC, the survival rate is significantly lower for SRCC as there are higher rates of localized peritoneal carcinomatosis and infiltrating tumors showing affinity for lymphatic tissue lymph node involvement.7
When tumor staging goes above TNM stage-I, studies have shown that prognosis becomes significantly worse for SRCC vs patients without SRCC.6,8 The infrequency and severity of perforation in gastric cancers makes it very challenging to predict the outcome in these cases.
It remains important to consider other unique patient factors when deciding on whether to pursue aggressive treatment with a total gastrectomy or stick to conservative therapy with either a simple closure with omental patch or a subtotal gastrectomy. The major determinants of improved survivability in patients with PGC are not only affected by the TNM stage and surgical approach chosen, but also the absence of pre-operative comorbidities and sepsis.9 Therefore, patients with cardio-respiratory illnesses or presence of sepsis may benefit from a stepwise surgical approach instead of a radical one.
A study examining 18 patients who underwent emergent surgery for PGC showed a significant correlation between the presence of comorbidities and mortality, as well as a significant correlation between sepsis status and mortality. The mean age for non-survivors was 63.1 years and 53.8 years for survivors.9
The positive post-operative outcome and success of the total gastrectomy in healing the perforation and relieving our patient’s symptoms sheds light on an atypical complication of a rare gastric cancer subtype that is scarcely documented. The patient’s long-term survival rate was optimally extended by radical resection of the stomach, and further management, including appropriate regional lymphadenectomy, could offer a high probability of cure.10
- Kong L, Yang N, Shi L, Zhao G, Wang M, Zhang Y. Total versus subtotal gastrectomy for distal gastric cancer: meta-analysis of randomized clinical trials. Onco Targets Ther. 2016;9:6795-6800. doi:10.2147/OTT.S110828.
- Zaafouri H, Jouini R, Khedhiri N, et al. Comparison between signet-ring cell carcinoma and non-signet-ring cell carcinoma of the stomach: clinicopathological parameters, epidemiological data, outcome, and prognosis-a cohort study of 123 patients from a non-endemic country. World J Surg Oncol. 2022;20(1):238. doi:10.1186/s12957-022-02699-8.
- Roviello F, Rossi S, Marrelli D, et al. Perforated gastric carcinoma: a report of 10 cases and review of the literature. World J Surg Oncol. 2006;4(19). doi:10.1186/1477-7819-4-19.
- Prueksapanich P, Pittayanon R, Wisedopas N, Rerknimitr R. A non-progressive signet patient with ring cell gastric adenocarcinoma who survived for 6 years without treatment. BMJ Case Rep. Published online July 9, 2013. https://doi.org/10.1136/bcr-2013-200365
- Ignjatovic N, Stojanov D, Djordjevic M, Ignjatovic J, Benedeto Stojanov D, Milojkovic B. Perforation of gastric cancer - what should the surgeon do? Bosn J Basic Med Sci. 2016;16(3):222-226. doi:10.17305/bjbms.2016.1020.
- Di Carlo S, Franceschilli M, Rossi P, et al. Perforated gastric cancer: a critical appraisal. Discov Oncol. 2021;12(15). doi:10.1007/s12672-021-00410
- Piessen G, Messager M, Leteurtre E, Jean-Pierre T, Mariette C. Signet ring cell histology is an independent predictor of poor prognosis in gastric adenocarcinoma regardless of tumoral clinical presentation. Ann Surg. 2009;250(6):878-887. doi:10.1097/SLA.0b013e3181b21c7b.
- Zhang C, Liu R, Zhang WH, et al. Difference between signet ring cell gastric cancers and non-signet ring cell gastric cancers: a systematic review and meta-analysis. Front Oncol. 2021;11:618477. doi:10.3389/fonc.2021.618477.
- Baykan M, Arikan TB, Donder Y, Sözüer E, Akyildiz HY. A perforated gastric carcinoma: a single-center experience. Int Surg. 2019;104(5-6):269-276. doi:10.9738/INTSURG-D-17-00069.1
- Machlowska J, Pucułek M, Sitarz M, Terlecki P, Maciejewski R, Sitarz R. State of the art for gastric signet ring cell carcinoma: from classification, prognosis, and genomic characteristics to specified treatments. Cancer Manag Res. 2019;11:2151—2161. doi:10.2147/CMAR.S188622.