
Peer Reviewed
Hepatic Vein Thrombosis: A Rare Cause of Fever of Unknown Origin
AUTHORS:
Ashley Ropell1 • Sandeep A. Gandhi, MD2
AFFILIATIONS:
1Medical Student, New York College of Osteopathic Medicine, New York, New York
2Infectious Disease Consultant, Northwell Health-Peconic Bay Medical Center, Riverhead, New York
CITATION:
Ropell A, Gandhi S. Hepatic vein thrombosis: a rare cause of fever of unknown origin. Consultant. 2022;62(7):e23-e25. doi:10.25270/con.2021.12.00009
Received May 26, 2021. Accepted July 12, 2021. Published online December 22, 2021.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Sandeep Gandhi, MD, Peconic Bay Medical Center, 1300 Roanoke Ave, Riverhead, NY 11901 (sanganmd@gmail.com)
A 60-year-old man with no significant medical history presented to our emergency department (ED) with a 5-week history of fevers and chills associated with night sweats, decreased appetite, and a 0.9-kg weight loss.
History. The patient denied any abdominal pain or other symptoms. No sick contacts or international travel history was reported. The patient denied any personal or family history of clotting disorders, COVID-19 infection or exposure, history of malignancy, or recent injury. He did not have a history of diverticulitis.
Three weeks prior to presentation, he had visited the same ED with similar symptoms. Laboratory studies conducted at that time had revealed elevated liver enzyme levels (aspartate aminotransferase level of 66 U/L, alanine aminotransferase level of 100 U/L) and no infection. He then followed up with his primary care physician, who had performed a magnetic resonance imaging (MRI) scan, revealing a complete right hepatic vein thrombosis. These findings prompted the primary care physician to recommend hospital admission the following day.
Physical examination. The patient was afebrile with tachycardia (103 beats/min). Other vital signs were within normal limits. Results of a physical examination were noncontributory, and all peripheral pulses were palpable. Pertinent negatives included no dental caries or ulcers, abdominal tenderness, ascites, hepatosplenomegaly, edema of the lower extremities, livedo reticularis, or jaundice.
Diagnostic testing. Significant laboratory study results included an elevated level of aspartate aminotransferase (72 U/L) and an elevated white blood cell count (27.75 × 103/uL), with a neutrophil predominance of 23,310/uL and bandemia, with a platelet count of 381 × 103/uL. The patient’s prothrombin time was elevated at 15.7 seconds, as well as an elevated activated partial thromboplastin time of 56.7 seconds. The results of a polymerase chain reaction test were negative for SARS-COV-2, and systemic inflammatory response syndrome criteria were fulfilled with an elevated heart rate of 103 beats/min and leukocytosis. A full sepsis workup was conducted, as well as a chest radiography scan, results of which showed no active parenchymal disease. The patient was admitted to the hospital for right hepatic vein thrombosis and fever of unknown origin.
An infectious disease specialist was consulted for possible septic thrombosis, and an oncologist was consulted for possible underlying malignancy. Tickborne illnesses were ruled out. In addition, test results were negative for COVID-19 spike protein antibody, COVID-19 capsid protein antibody, and antiplatelet factor 4 antibody. Upon further examination, no hematologic malignancy was suspected, and the patient was counseled on follow-up cancer screening as an outpatient.
Treatment. Intravenous fluids were administered, and a heparin protocol was initiated. The patient was administered one dose of enoxaparin sodium, 100 mg subcutaneously, piperacillin/tazobactam, 3.375 g/100 mL intravenously, and acetaminophen as needed for fevers.
A bedside echocardiogram raised suspicion for vegetation of the anterior mitral valve leaflet. A computed tomography scan of the chest, abdomen, and pelvis revealed thrombosis of the right hepatic vein confirming results seen on the prior MRI scan, as well as diverticulosis with possible diverticular abscess at the level of the sigmoid colon (Figure 1).

A general surgeon was consulted and suggested a possible episode of diverticulitis at the onset of symptoms that led to the translocation of bacteria. Blood cultures that were negative at the prior ED visit were now growing Streptococcus anginosus. The patient’s antibiotic regimen was switched to ampicillin/sulbactam, 3 g/100 mL intravenously every 6 hours.
Patient outcome. During his hospital course, the patient remained mostly afebrile, except for an occasional temperature spike of 39 °C, with normal physical examination findings. A transesophageal echocardiogram was performed to rule out vegetations, results of which did not show any abnormalities. Further blood cultures grew Streptococcus constellatus, which was treated with the same antibiotic. Negative cultures were achieved by hospital day 5.
A repeat computed tomography scan showed resolution of the possible diverticular abscess and resembled chronic diverticular disease with no complications, as well as a complete right hepatic vein thrombosis unchanged from the initial study (Figure 2). An interventional radiologist was not consulted for drainage at the time but will be consulted if the patient does not clinically improve or if the abscess persists.

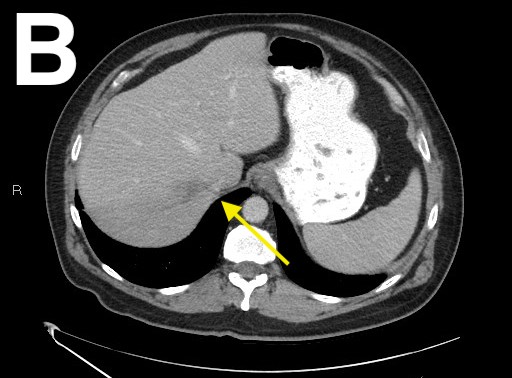


Figure 2. A computed tomography scan of the abdomen and pelvis showed an unchanged right hepatic vein thrombosis (A-C) and a resolved diverticular abscess (D).
The patient was discharged home with a peripherally inserted central catheter to receive intravenous ceftriaxone, 1 g daily for 5 days. He also was prescribed metronidazole, 500 mg orally every 8 hours for 5 days. He was discharged after a 1-week hospital stay and instructed to follow up with a hematologist as an outpatient for hypercoagulable work-up, as well as with his primary care physician for routine cancer screening including prostate cancer screening and colonoscopy.
Discussion. Budd-Chiari syndrome is characterized by a reduced blood flow to the liver. The incidence is 0.1 to 10.0 per million people per year, with etiologies including hypercoagulable conditions, myeloproliferative diseases, anatomical variations of the inferior vena cava, and environmental triggers.1 About 80% of reported cases have a secondary cause such as malignancy or trauma.2 The survival rate is 42% to 100% in treated patients depending on etiology, risk factors, and choice of treatment.1 In the case of an infective thrombosis of the portal vein, or pylephlebitis, the diagnosis requires high suspicion, as presenting symptoms are nonspecific and pylephlebitis has a high mortality rate of 25%.3 Pylephlebitis is a rare disorder that can complicate infections of the gastrointestinal tract and occurs as a complication of diverticulitis in 3% of cases.3 The risk factors for this condition include diverticulitis, appendicitis, inflammatory bowel disease, pancreatitis, infectious enteritis, and recent abdominal surgery.3 Appendectomies are a common etiology of portal vein thrombosis.4 An intra-abdominal infection can result in suppurative thrombophlebitis, resulting in pylephebitits.4 However, in approximately 70% of cases, no underlying etiology can be identified.3
In a 1995 study, researchers reviewed 19 cases of pylephlebitis published since 1979 and investigated diagnostic and management issues of pylephlebitis.5 Pylephlebitis occurs when intestinal bacteria gets transported to the portal circulation. A common precipitating factor is diverticulitis.5 these reported cases, 88% of them had led to bacteremia, and the overall mortality rate was 32%.5
Upon presentation to the emergency department, many patients report fever for extended periods of time and abdominal pain. They may also present with an acute abdomen, ascites, and jaundice. In almost 20% of cases, it is even revealed by severe sepsis.4 Conversely, an individual may be completely asymptomatic.3 Patients typically are found to have leukocytosis, abnormal liver function test results, and may even show pathologic changes on imaging of the liver including intense congestion, cell necrosis, and inflammatory reactions. A definitive diagnosis is made by catheterization of the hepatic veins and/or inferior vena cava. 6
Of note, growth in blood cultures occurs in 50% to 80% of patients with pylenphlebitis.4Escherichia coli and Streptococcus species have been identified as the most common organisms.4 Other infectious agents include Bacteroides fragilis, Viridans streptococci, Proteus mirabilis, and Klebsiella pneumoniae.4 Death occurs from sepsis, peritonitis, intestinal bleeding, or a portal vein rupture.3 Recommended antibiotic regimens include piperacillin/tazobactam, quinolones, or metronidazole.3 Treatments should include a combination of antibiotics and anticoagulants. Anticoagulation is generally recommended for 3 to 6 months to prevent thrombus extension and to promote recanalization.3 Surgical intervention is rarely necessary but may be warranted for either the thrombus or the primary infection site (ie, appendix or diverticular abscess). If left untreated, portal hypertension may occur.4
References
1. Grus T, Lambert L, Grusová G, Banerjee R, Burgetová A. Budd-Chiari syndrome. Prague Med Rep. 2017;118(2-3):69-80. https://doi.org/10.14712/23362936.2017.6
2. Kubo H, Asai G, Haraguchi K, et al. Liver abscess and portal vein thrombosis due to ileal diverticulitis mediated by barium fluoroscopy. Intern Med. 2017;56(23):3255-3259. https://doi.org/10.2169/internalmedicine.9223-17
3. Cheesman AR, Gremida A, Burton M. Acute infective portal vein thrombosis secondary to acute sigmoid diverticulitis. J Gastroenterol Hepatol Res. 2015;4(4):1582-1584. http://www.ghrnet.org/index.php/joghr/article/view/1066/1263
4. Faisal El mouhafid, Noueddine Njoumi, Mohamed Najih, Yasser, Brahmi, Mohamed Friha, Hicham Iraki, Abdelkader Ihirchiou, Aziz Zentar. Portal vein thrombosis as revealed by a post-appendicectomy abscess. About a case. J Surg Res. 2018;1:58-62. https://www.fortunejournals.com/articles/pportal-vein-thrombosis-as-revealed-by-a-postappendicectomy-abscess-about-a-casep.html
5. Plemmons RM, Dooley DP, Longfield RN. Septic thrombophlebitis of the portal vein (pylephlebitis): diagnosis and management in the modern era. Clin Infect Dis. 1995;21(5):1114-1120. https://doi.org/10.1093/clinids/21.5.1114
6. Maddrey WC. Hepatic vein thrombosis (Budd-Chiari syndrome). Hepatology. 1984;4(1 Suppl):44S-46S. https://doi.org/10.1002/hep.1840040713