
An Atlas of Lumps and Bumps: Part 25
AFFILIATIONS
1Clinical Professor of Pediatrics, the University of Calgary
2Pediatric Consultant, the Alberta Children’s Hospital, Calgary, Alberta, Canada
3Dermatologist, Medical Director and Founder, the Toronto Dermatology Centre, Toronto, Ontario, Canada
4Associate Clinical Professor of Pediatrics, Dermatology and Skin Sciences, the University of British Columbia, Vancouver, British Columbia, Canada
5Pediatric Dermatologist, the Pediatric Institute, Kuala Lumpur General Hospital, Kuala Lumpur, Malaysi
CITATION
Leung AKC, Barankin B, Lam JM, Leong KF. An atlas of lumps and bumps, part 25. Consultant. 2023;63(3):e10. doi:10.25270/con.2023.03.000006.
DISCLOSURES
Dr Leung is the series editor. He was not involved with the handling of this paper, which was sent out for independent external peer review.
CORRESPONDENCE
Alexander K. C. Leung, MD, #200, 233 16th Ave NW, Calgary, AB T2M 0H5, Canada (aleung@ucalgary.ca)
EDITOR’S NOTE
This article is part of a series describing and differentiating dermatologic lumps and bumps. To access previously published articles in the series, visit https://www.consultant360.com/resource-center/atlas-lumps-and-bumps.
Lipoma
A lipoma is a benign tumor composed of collections of mature adipocytes enclosed by a thin, fibrous capsule. It is, by far, the most common mesenchymal neoplasm and accounts for approximately 50% of all soft-tissue tumors.1 Although lipomas have been reported in virtually all organs such as the kidneys, liver, gastrointestinal tract, heart, and lungs, they occur most frequently in the subcutaneous tissue.2-4
It is estimated that lipomas occur in 0.2 to 1% of the adult population.5,6 The peak incidence is between 40 and 60 years of age.3,6,7 Children and young adults and children also can be affected.3,6,7 In general, solitary lipomas are more common in females whereas multiple lipomas are more common in males.2,4 The condition is usually sporadic, although familial cases have also been reported.8 Risk factors include obesity, alcoholism, diabetes mellitus, hyperlipidemia, liver disease, and use of protease inhibitors in patients with HIV.9-11
The exact etiopathogenesis is not known. Trauma (especially blunt trauma) is implicated in the pathogenesis at least in some cases.5 It is believed that rupture of the fibrous septa and anchorage connections between the skin and deep fascia after trauma may result in proliferation of adipose tissue.11,12 Also, trauma may induce cytokine release that may trigger preadipocytes differentiation and maturation.11 Genetic predisposition also plays a role as clonal chromosomal aberrations are not uncommon in patients with lipomas.13,14 Lipomas may result from a mutation in the HMGA2-LPP fusion gene located on chromosome (12q14.3).14NFIB is the target gene in deep-seated lipomas with 9p22-24 rearrangements.14 Other cytogenetic abnormities that have been identified include deletion of 13q and rearrangements of 6p21-33.10
Clinically, a lipoma presents as a slow-growing, soft, well-circumscribed, lobulated, oval or round, dome-shaped or egg-shaped subcutaneous nodule that is not attached to the overlying skin or underlying structures (Figures 1 to 3).

Fig. 1 A lipoma on a patient's back is shown.

Fig. 2 A lipoma on a patient's forearm is shown.

Fig. 3 A lipoma on a patient's forehead is shown.
The overlying skin is characteristically normal. A characteristic "slipping sign" may be elicited by gently sliding the fingers off the edge of the tumor (Figure 4A-B).10


Fig. 4A-B A characteristic "slipping sign" is shown.
The tumor will be felt to slip out from under the fingers. The size of a lipoma usually ranges from 2 to 5 cm in diameter.11,15 Occasionally, lipomas can be greater than 10 cm in diameter and are referred to as “giant lipomas”10,16 Sites of predilection include the back, posterior neck, shoulders, proximal portions of extremities (especially the upper extremities), abdomen, and buttocks.7,11 Most lipomas are asymptomatic and solitary.2,3,11 Multiple lipomas (Figures 5) occur in approximately 5% of all cases.6,11
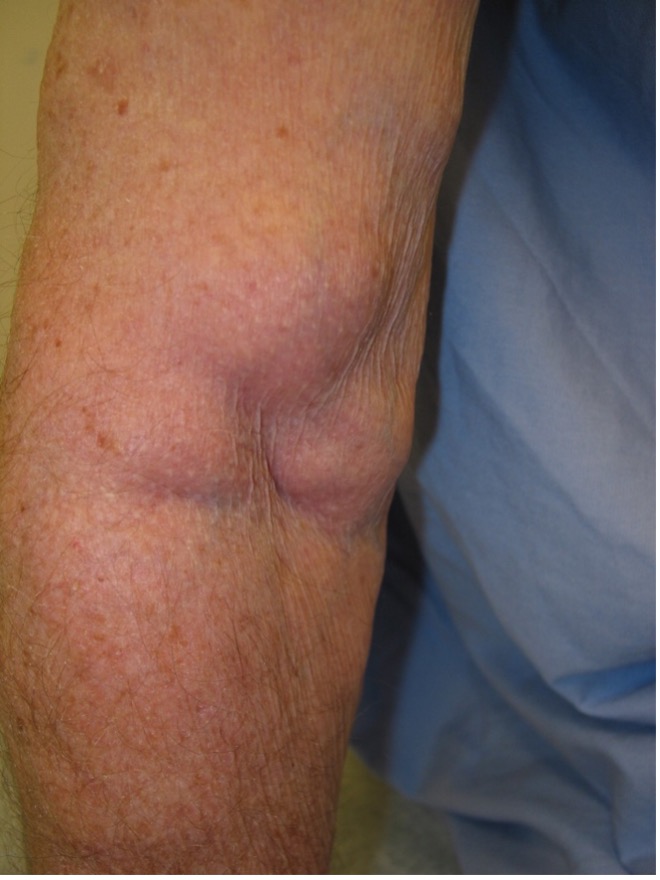
Fig. 5 An arm with multiple lipomas is shown.
Rarely, lipomas, especially when multiple, may be associated with Gardner syndrome, Cowden syndrome, Proteus syndrome, Bannayan-Riley-Ruvalcaba syndrome, Pai syndrome, benign symmetric lipomatosis (Madelung disease), Dercum disease, adiposis dolorosa, congenital lipomatosis, and familial multiple lipomatosis.3,6,11,13,17,18
A lipoma may be cosmetically unsightly and may have an adverse effect on quality of life.18 Depression disorders are more common in patients with multiple lipomas or lipomas of considerable size.11 Other uncommon complications include infection, fatty necrosis, xanthomatous change, calcifications, ulceration, gangrene, and compression of adjacent structures or of a peripheral nerve.15,19 Carpal tunnel syndrome is one of the most common compression neuropathies.1,19,20 Compression fracture of vertebral bones has rarely been reported.21 Lipomas in other locations may cause pain, dysphagia, breathing difficulties, cardiac arrhythmia, or intestinal obstruction. A lipoma in the lumbosacral area may be a cutaneous marker of occult lumbosacral dysraphism.2 Liposarcoma usually arise de novo and malignant transformation from a pre-existing lipoma is rare.18,21,23
The diagnosis is mainly clinical. No imaging studies are usually required. Plain radiographs typically demonstrate lucency in the soft tissue consistent with fat. Imaging studies using ultrasonography, magnetic resonance imaging or computed tomography may be considered if the lipoma is large, has atypical features, or appears in deeper structures. A skin biopsy for histology should be considered if the diagnosis is in doubt.
1. Barreira M, Marques N, Campos V, Marques G, Gonçalves S, Stefanova Alves S. A giant hand lipoma as a rare cause of secondary carpal tunnel syndrome - A case report. Int J Surg Case Rep. 2020;77:538-542. doi:10.1016/j.ijscr.2020.11.083.
2. Aydogdu E, Yyldyrym S, Eker G, Aköz T. Giant lipoma of the back. Dermatol Surg. 2004;30(1):121-122.
3. Nguyen T, Zuniga R. Skin conditions: benign nodular skin lesions. FP Essent. 2013;407:24-30.
4. Richert B, Andre J, Choffray A, Rahier S, de la Brassinne M. Periungual lipoma: about three cases. J Am Acad Dermatol. 2004;51(2 Suppl):S91-93. doi:10.1016/j.jaad.2003.12.051.
5. Copcu E. Sport-induced lipoma. Int J sports Med. 2004;25(3):182-185. doi:10.1055/s-2003-45254.
6. Pandya KA, Radke F. Benign skin lesions: lipomas, epidermal inclusion cysts, muscle and nerve biopsies. Surg Clin North Am. 2009;89(3):677-687. doi:10.1016/j.suc.2009.03.002.
7. Jayi S, Laadioui M, Fatemi HE, Fdili FZ, Bouguern H, Chaara H, et al. Vulvar lipoma: a case report. J Med Case Rep. 2014 June 18;8:203. doi:10.1186/1752-1947-8-203.
8. Toy BR. Familial multiple lipomatosis. Dermatol Online J. 2003;9(4):9.
9. Choi HS, Yi JH, Kang SH, Yun SK. Lipoma of the index finger. J Dermatol. 2003;30(11):834-836. doi:10.1111/j.1346-8138.2003.tb00487.x.
10. Kolb L, Yarrarapu SNS, Ameer MA, Rosario-Collazo JA. Lipoma. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan–2020 Oct 6.
11. Szewc M, Gawlik P, Żebrowski R, Sitarz R. Giant lipoma in the fronto-temporo-parietal region in an adult man: Case report and literature review. Clin Cosmet Investig Dermatol. 2020;13:1015-1020. doi:10.2147/CCID.S273189.
12. Nakamura Y, Teramoto Y, Sato S, Yamada K, Nakamura Y, Fujisawa Y, et al. Axillary giant lipoma: a report of two cases and published work review. J Dermatol. 2014;41(9):841-844. doi:10.1111/1346-8138.12598.
13. Erickson LA. Lipoma. Mayo Clin Proc. 2019;94(1):176-177. doi:10.1016/j.mayocp.2018.11.007.
14. Italiano A, Ebran N, Attias R, Chevallier A, Monticelli I, Mainguené C, et al. NFIB rearrangements in superficial, retroperitoneal, and colonic lipomas with aberrations involving chromosome band 9p22. Genes Chromosomes Cancer. 2008;47(11):971-977. doi:10.1002/gcc.20602.
15. Sanchez M, Golomb FM, Moy JA, Potozkin JR. Giant lipoma: case report and review of the literature. J Am Acad Dermatol. 1993;28(2):266-268. doi:10.1016/s0190-9622(08)81151-6.
16. Litchinko A, Cherbanyk F, Menth M, Egger B. Giant gluteal lipoma surgical management. BMJ Case Rep. 2019;12(8):e229842. doi:10.1136/bcr-2019-229842.
17. Buisson P, Leclair MD, Jacquemont S, Podevin G, Camby C, David A. Cutaneous lipoma in children: 5 cases with Bannayan-Riley-Ruvalcaba syndrome. J Pediatr Surg. 2006;41(9):1601-1603. doi:10.1016/j.jpedsurg.2006.05.013.
18. Savasta S, Chiapedi S, Perrini S, Tognato E, Corsano L, Chiara A. Pai syndrome: a further report of a case with bifid nose, lipoma, and agenesis of the corpus callosum. Childs Nerv Syst. 2008;24(6):773-776. doi:10.1007/s00381-008-0613-9.
19. Unal M, Demirayak E, Acar B, Kose O. Simultaneous median and ulnar compression neuropathy secondary to a giant palmar lipoma: A case report and review of the literature. Cureus. 2018;10(2):e2198. doi:10.7759/cureus.2198.
20. Ribeiro G, Salgueiro M, Andrade M, Fernandes VS. Giant palmar lipoma - an unusual cause of carpal tunnel syndrome. Rev Bras Ortop. 2017;52(5):612-615. doi: 10.1016/j.rboe.2017.08.001.
21. Kino H, Sugita N, Akamatsu J, Mitsuno D, Ueda K. Giant lipoma of the back caused compression fracture of the thoracic vertebral bones. Plast Reconstr Surg Glob Open. 2019 May 3;7(5):e2232. doi:10.1097/GOX.0000000000002232.
22. Taviere V, Brunelle F, Baraton J, Temam M, Pierre-Kahn A, Lallemand D. MRI study of lumbosacral lipoma in children. Pediatr Radiol. 1989;19(5):316-320. doi:10.1007/BF02467302.
23. Temelkova I, Wollina U, Di Nardo V, Tchernev G. Lipoma of the neck. Open Access Maced J Med Sci. 2018;6(10):1875-1877. doi:10.3889/oamjms.2018.430.