
Peer Reviewed
Skin Disorders in Older Adults: Eczematous and Xerotic Inflammatory Conditions, Part 2
AUTHOR:
Noah S. Scheinfeld, MD, JD
Columbia University
CITATION:
Scheinfeld NS. Skin disorders in older adults: eczematous and xerotic inflammatory conditions, part 2. Consultant. 2010;50(9):388-393.
ABSTRACT: Eczematous and xerotic inflammatory dermatoses are more common in older adults because of the impairment in epidermal integrity that occurs with aging. Stasis dermatitis usually affects the lower extremities, often in areas of long-standing venous insufficiency, and occurs more frequently in women than in men. Support stockings, elastic wraps, and Unna boots are examples of compression devices that can be used to mitigate the effects of venous insufficiency. In elderly persons, irritant contact dermatitis is often caused by topical medications. The dermatitis responds well to bland, topical corticosteroids; however, the only truly effective treatment is avoidance. Treatment of allergic contact dermatitis involves identification of the allergen with patch testing and avoidance of it. Immediate symptoms can be treated with topical corticosteroids.
Key words: stasis dermatitis, irritant contact dermatitis, allergic contact dermatitis
Because the immune response declines with age, most inflammatory skin diseases are less common in older adults than in younger persons.1 However, eczematous and xerotic inflammatory dermatoses are more prevalent among persons older than 60 years as a result of the impairment in epidermal integrity that occurs with aging.
In this 2-part series, I focus on the diagnosis and treatment of these dermatoses in older adults. Here I discuss stasis dermatitis, irritant contact dermatitis, and allergic contact dermatitis. In a previous issue (CONSULTANT, June 2010, page 239), I addressed seborrheic dermatitis, xerosis, asteatotic eczema, and nummular dermatitis
STASIS DERMATITIS
Etiology. The etiology of stasis dermatitis is complex. Alteration of deep venous plexus function of the leg leads to the backflow of blood to the superficial venous system, which causes venous hypertension and cutaneous inflammation.
Clinical features. Stasis dermatitis usually affects the lower extremities, often in areas of long-standing venous insufficiency, and is more common in women. The bilateral circumferential dermatitis is characterized by lichenified and hyperpigmented plaques on the ankle and calf areas (Figure 1). The triad of alopecia, waxy appearance, and yellow-brown pigment from hemosiderin deposition is highly specific for stasis dermatitis with or without pitting edema (Figure 2). Secondary infection can develop (Figure 3). Ulcerations may also occur (Figure 4). Stasis dermatitis can be misdiagnosed as cellulitis.

Figure 1. Stasis dermatitis is seen here on the leg of an elderly woman. This bilateral circumferential dermatitis is characterized by lichenified and hyperpigmented plaques.

Figure 2. Xerosis and stasis dermatitis coexist on the leg of this elderly woman.

Figure 3. Secondary infection of stasis dermatitis has occurred on the legs of this elderly woman.

Figure 4. Ulcers have developed on the leg of this patient with stasis dermatitis.
Rarely, stasis dermatitis is associated with the development of violaceous plaques and nodules on the legs and dorsal part of the feet, which resemble classic Kaposi sarcoma (Figure 5). As a result, this manifestation has been called pseudo–Kaposi sarcoma, or acroangiodermatitis.
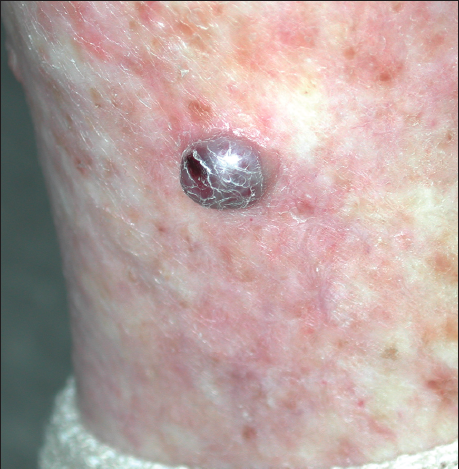
Figure 5. This violaceous nodule resembles classic Kaposi sarcoma but is actually a rare manifestation of stasis dermatitis, which has been called pseudo–Kaposi sarcoma, or acroangiodermatitis.
In immobile elderly patients, stasis dermatitis–like eruptions and pressure ulcers can occur at sites other than the legs, such as the buttocks, heels, forearms, and any other body area that rests on a solid surface and is exposed to long-term pressure.
Treatment. The goal of treatment is to mitigate the effects of venous insufficiency. Consider ordering venous Doppler studies to determine whether vascular surgery is needed. Compression therapy can be administered to control the amount of pressure on the legs. Support stockings, elastic wraps, and Unna boots are examples of devices that can be used on affected legs. Both regular exercise and elevation of the legs 6 inches above the heart have been shown to be effective treatment measures.2
Topical corticosteroids used to treat stasis dermatitis can cause infection if the patient has open excoriations. Topical antibiotics, such as mupirocin, should also be used. Avoid bacitracin, which can cause contact dermatitis.3
IRRITANT CONTACT DERMATITIS
Clinical features. In elderly persons, irritant contact dermatitis is commonly caused by topical medications. It develops as a response to chemical damage to the epidermis and presents as an inflammation of the skin with varying degrees of erythema, edema, and scaling (Figure 6). Irritant contact dermatitis does not spread beyond the initial area of application.

Figure 6. Irritant contact dermatitis developed in this elderly woman as a result of long-term use of topical medications to treat stasis dermatitis.
In the United States, irritant contact dermatitis is common in persons who constantly expose their skin to water or other irritants, and it is seen more frequently in women, probably from exposure to cleaning products.4 Irritants such as detergents and solvents strip protective oils from the skin. Strong irritants produce immediate reactions, while mild irritants require longer exposure before a reaction develops. Initial symptoms include warmth, burning, and stinging.
Secondary infections can occur, particularly with Staphylococcus aureus. A skin biopsy can be done to exclude other disorders, such as psoriasis.
Treatment. Irritant contact dermatitis responds well to bland, topical corticosteroids, such as triamcinolone 0.025% ointment in a pure petrolatum base. Ultimately, the only truly effective treatment is avoidance of the irritating substance.
ALLERGIC CONTACT DERMATITIS
Clinical features. Allergic contact dermatitis is characterized by erythema, edema, and vesiculation. This delayed type of induced sensitivity results from cutaneous contact with an allergen to which the patient has a specific sensitivity. The dermatitis occurs at sites where substances or metals have been applied (Figure 7). In elderly persons, the development of allergic contact dermatitis may be delayed somewhat, but the dermatitis may be more persistent once it occurs.5
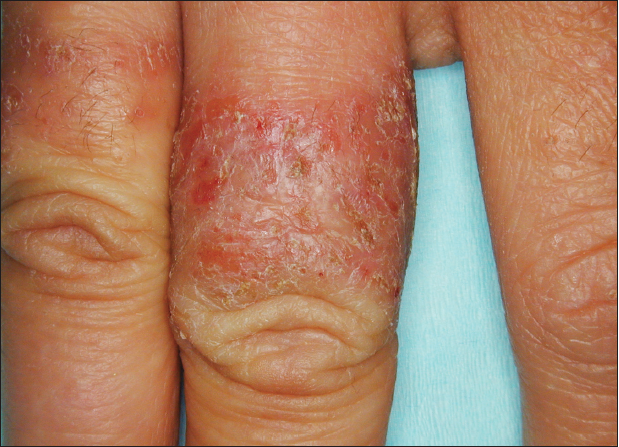
Figure 7. The pattern of erythema, vesiculation, and edema on this man’s finger suggests allergic contact dermatitis. The suspected culprit was nickel in the ring he habitually wore.
Treatment. This involves identification of the allergen with patch testing and avoidance of it. Immediate symptoms can be treated with topical corticosteroids.
Patients with stasis dermatitis are at high risk for the development of allergic contact dermatitis to materials and agents applied to the areas of stasis dermatitis and leg ulcers. Neomycin is an important cause of allergic contact dermatitis in these persons because it is used frequently despite the lack of documentation of its efficacy in the treatment of stasis ulcers.6
Dr Scheinfeld is assistant clinical professor of dermatology at Columbia University and assistant attending physician at St Luke’s–Roosevelt and Beth Israel Hospitals in New York.
REFERENCES:
1. Nedorost ST, Stevens SR. Diagnosis and treatment of allergic skin disorders in the elderly. Drugs Aging. 2001;18:827-835.
2. Collins L, Seraj S. Diagnosis and treatment of venous ulcers. Am Fam Physician. 2010;81:989-996.
3. Jacob SE, James WD. From road rash to top allergen in a flash: bacitracin. Dermatol Surg. 2004;30(4, pt 1):521-524.
4. Dickel H, Kuss O, Schmidt A, et al. Importance of irritant contact dermatitis in occupational skin disease. Am J Clin Dermatol. 2002;3:283-289.
5. Tosti A, Pazzaglia M, Silvani S, Delorenzi F. The spectrum of allergic contact dermatitis in the elderly. Contact Dermatitis. 2004;50:379-381.
6. Hogan DJ. Widespread dermatitis after topical treatment of chronic leg ulcers and stasis dermatitis. CMAJ. 1988;138:336-338.
1. Nedorost ST, Stevens SR. Diagnosis and treatment of allergic skin disorders in the elderly. Drugs Aging. 2001;18:827-835.
2. Collins L, Seraj S. Diagnosis and treatment of venous ulcers. Am Fam Physician. 2010;81:989-996.
3. Jacob SE, James WD. From road rash to top allergen in a flash: bacitracin. Dermatol Surg. 2004; 30(4, pt 1):521-524.
4. Dickel H, Kuss O, Schmidt A, et al. Importance of irritant contact dermatitis in occupational skin disease. Am J Clin Dermatol. 2002;3:283-289.
5. Tosti A, Pazzaglia M, Silvani S, Delorenzi F. The spectrum of allergic contact dermatitis in the elderly. Contact Dermatitis. 2004;50:379-381.
6. Hogan DJ. Widespread dermatitis after topical treatment of chronic leg ulcers and stasis dermatitis. CMAJ. 1988;138:336-338.