
Peer Reviewed
Superior Mesenteric Vein Thrombosis Associated With Oral Contraceptive Use
AUTHORS:
Alan Lucerna, DO1 • James Espinosa, MD1 • Wayne Tamaska, DO1 • Risha Hertz, APNC2 • Douglas Stranges, DO3 • Anthony DiPasquale, DO1
AFFILIATIONS:
1Department of Emergency Medicine, Rowan University School of Medicine/Jefferson Health, Stratford, New Jersey
2Penn Medicine, Gibbsboro, New Jersey
3Virtua Hospital, Vorhees, New Jersey
CITATION:
Lucerna A, Espinosa J, Tamaska W, Hertz R, Stranges D, DiPasquale A. Superior mesenteric vein thrombosis associated with oral contraception use. Consultant. 2022;62(1):e22-e25. doi:10.25270/con.2021.04.00011
Received November 22, 2020. Accepted January 18, 2021. Published online April 21, 2021.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Alan Lucerna, DO, Department of Emergency Medicine, Rowan University, 18 East Laurel Road, Stratford, NJ 08084 (lucernaa@gmail.com)
A 24-year-old woman presented to our emergency department (ED) with a 1-week history of intermittent abdominal pain. The pain was predominantly located in the epigastric region with some radiation into her back with no associated nausea, vomiting, fevers, chills, or diarrhea. She denied stool changes, and she did not notice any blood in her urine or stools.
The patient had no significant medical or surgical history. She did not smoke or take any illicit drugs. Her family history was notable for her brother who had a deep vein thrombosis and a grandmother who had a pulmonary embolus. The patient had no history of blood clots. She did not report any recent travel or any prolonged immobility or trauma. The only medication she was taking was an oral contraceptive that contained desogestrel (progestin), 0.15 mg, and ethinyl estradiol (estrogen), 0.03 mg, to help control her painful menses.
On arrival to the ED, her vital signs were as follows: oral temperature of 36.8 °C, heart rate of 57 bpm, blood pressure of 132/62 mm Hg, respiratory rate of 18 br/min, and a pulse oximetry of 99% on room air.
Physical examination. Notable findings included tenderness to palpation at the epigastric region, but her abdomen did not show signs of peritonitis. All quadrants were soft, with good bowel sounds. Her abdomen was not distended. Results of a complete blood cell count, basic metabolic panel, and liver function tests were all within normal limits.
Diagnostic testing. Because of the location of the pain, an ultrasonography scan of the right upper quadrant was conducted, results of which showed an increased echogenicity about the intrahepatic portal venous system but no sonographic evidence of cholelithiasis or acute cholecystitis.
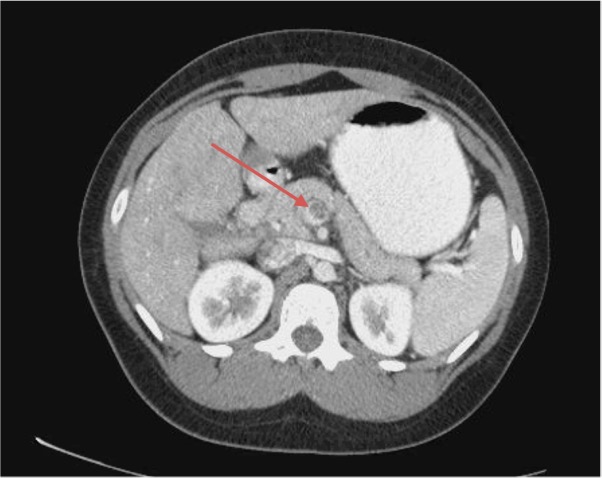
The patient had persistent pain upon reexamination, so a computed tomography (CT) scan of the abdomen and pelvis with oral and intravenous contrasts was conducted. Results revealed a thrombosed superior mesenteric vein and peripheral branches with retroperitoneal fat stranding about the vessel, which was compatible with thrombophlebitis (Figures 1 and 2). The transverse descending and proximal sigmoid colons were also mildly thickened, which was suspected to be more related to underdistention.

The patient was then placed on a heparin drip. During the course of her hospitalization, she was seen by a vascular surgeon, gastroenterologist, and hematologist. Her course was unremarkable, and her symptoms had improved. She was subsequently discharged home on rivaroxaban, 15 mg, twice daily, then 20 mg daily for 3 to 6 months. The results of a hypercoagulable panel were unremarkable. The superior mesenteric vein thrombosis (MVT) was attributed to oral contraceptive use. She was instructed to avoid taking oral contraceptives in the future and to follow-up with her gynecologist for alternate means of treatment for her painful menses.
Discussion. According to the Centers for Disease Control and Prevention, abdominal pain is the most common principal reason for ED visits in the United States, representing as many as 7.8% of all ED visits.1 Astute history taking, physical examination skills, and appropriate utilization of resources aid the ED physician in risk-stratifying patients to acute and nonacute abdominal pain and in making a diagnosis of MVT, which may be life-threatening.2,3
First described in 1895, MVT can lead to bowel infarction and is, therefore, potentially life-threatening.4,5 MVT is a rare medical emergency, accounting for only 5% of all cases of acute mesenteric ischemia. In comparison, acute mesenteric arterial thrombosis is attributed in 60% to 70% of cases.6
However, the challenge with diagnosing MVT is that the presenting symptoms can be subtle, nonspecific, and can evolve over the course of hours to weeks, which may cause a delayed diagnosis.4,5,7 The most common presenting symptom is colicky abdominal pain.6 Abdominal distention, nausea, vomiting, anorexia, and gastrointestinal bleeding have also been described.4,5,7 Therefore, a high degree of suspicion is needed, especially in patients with risk factors. The nonspecific and nonlocalizing features may be due to the variable amount of clot burden and its impact on the bowel circulation.8
Thrombotic complications from oral contraceptives are well known. The first case of mesenteric thrombosis associated with an oral contraceptive was reported in 1963.4,9 Oral contraceptives are thought to cause about 4% to 5% of all cases of MVT.4 Among women taking a combination of progestin and estrogen, as in the case of our patient, the thrombosis is thought to be associated with estrogen and the dose used. Thrombogenicity, therefore, decreases with lowering the estrogen dose and shortening the length of use.4,10 Within 1 month of discontinuation of oral contraceptives, the thrombotic risk decreases to baseline.4
While taking an oral contraceptive, the risk of clotting events is amplified further by increased age, tobacco use, hypercoagulable states, hereditary or acquired coagulopathy, surgery, connective tissue disease, and hypertension.4
However, among women with no risk factors, predicting who will develop thromboembolic events is unclear. Warshauer and colleagues have reported that 9 of their 42 patients (21%) with MVT had idiopathic causes, and in their review of the literature, they found that the idiopathic rate ranged from 19% to 46% overall.8
The mechanisms by which oral contraceptives induce hypercoagulable states may include the following:4
- Acceleration of the internal and external pathways of the coagulation cascade or by reduction of antithrombin III levels
- Induction of antifibrinolytic activity by decreasing spontaneous fibrinolysis
- Promotion of intimal hyperplasia
When taken with estrogen, progestin amplifies the effects of estrogen on procoagulant, anticoagulant, and fibrinolytic pathways.9
Other conditions that can cause MVT include pancreatitis, intra-abdominal sepsis, cirrhosis, portal hypertension, neoplasms, and blunt abdominal trauma.5
Because of nonspecific presenting symptoms and the lack of characteristic laboratory abnormalities or distinct physical examination findings, a contrast-enhanced CT scan of the abdomen may be conducted—not primarily looking for mesenteric ischemia but in the pursuit of the undifferentiated abdominal pain. Other times, MVT has been diagnosed in serendipity, as it has been previously reported to mimic appendicitis.11 Katagiri and colleagues have reported diagnosing MVT after a CT scan of the abdomen was conducted as a follow-up imaging test when the patient reported persistent anorexia after laparoscopic surgery.5 Nonetheless, the sensitivity of a contrast-enhanced CT scan of the abdomen and pelvis is about 90% to 100% sensitive and remains the imaging test of choice in diagnosing MVT.10,11 It not only facilitates early detection but also aids in determining between medical and operative management by providing anatomical indicators of intestinal viability and whether early or late signs of infarction, transmural, and nontransmural ischemia are present.10-12 Portal venous phase CT has been reported to have positive and negative predictive values of 100% and 94%.12
The CT findings may reveal central lucency in the mesenteric vein, enlargement of the superior mesenteric vein, a sharply defined vein wall with a rim of increased density, as well as intestinal edema.5 Intramural gas typical of bowel gangrene has also been described.12
While a magnetic resonance imaging scan has similar sensitivity to a CT scan, it is not readily available and has a higher cost. A Doppler ultrasonography scan has also been used to evaluate the flow in the mesenteric and portal venous systems, but the sensitivity is reportedly around 73% to 80%.11
Treatment and management. There is no consensus on what the optimal treatment is for acute MVT. Prevention of thrombus propagation through systemic anticoagulation is currently a well-used treatment option and a mainstay of treatment in patients with acute MVT.13
Involvement of surgical services is recommended, as peritoneal signs may not strictly correlate with the severity of bowel ischemia. In patients with bowel-wall thickness and bowel-wall enhancement on the arterial phase of CT, patient outcomes were improved with early surgical involvement.13
Koyama9 has described great success with early catheter-directed thrombolysis as an effective measure to forestall intestinal infarction. Catheter-directed thrombolytic therapy to reach the portal venous system through percutaneous transhepatic, transjugular transhepatic, and transaortic superior mesenteric artery has been reported.12
Surgery is indicated when clinical findings are consistent with peritonitis or when the imaging studies reveal bowel infarction or perforation.8 Thrombectomy as well as resection of the affected bowel have been also described.8-10
Abdominal physical findings, such as pain out of proportion to the examination, as well as imaging studies showing bowel ischemia or infarction can lead to negative outcomes, especially in patients with advanced age.8,11
Conclusion. Undifferentiated abdominal pain is a common presentation in the ED. MVT, although rare, should be considered, especially in patients taking an oral contraceptive, since MVT may lead to bowel ischemia and perforation. Contrast-enhanced CT scan is the imaging test of choice, but other imaging modalities have also aided diagnosis. Systemic anticoagulation is a well-recognized and well-used treatment option. Early involvement of surgical service is recommended.
Patient outcome. Our patient did well on systemic anticoagulation and did not require any surgical intervention. However, a vascular surgeon was involved with her case because her initial presentation caused concern.
References
1. Patterson JW, Kashyap S, Dominique E. Acute Abdomen. In: StatPearls [Internet]. StatPearls Publishing; 2021. https://www.ncbi.nlm.nih.gov/books/NBK459328/
2. Smith KA. Abdominal pain. In: Marx J, Hockberger R, Walls R, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 8th ed. Saunders; 2013:213-223.
3. Brunetti R, David C, Richards L, McCarthy MJ, Meltzer AC. Severity of pain is not associated with urgency of diagnosis in ED patients with abdominal pain. Presented at: GW Research Days 2016; March 29-30, 2016; Washington DC. https://hsrc.himmelfarb.gwu.edu/gw_research_days/2016/SMHS/125/
4. Stewart H, Flannery MT, Humphrey DA. Superior mesenteric vein thrombosis secondary to oral contraceptive use. Case Rep Vasc Med. 2012;2012. https://doi.org/10.1155/2012/969130
5. Katagiri H, Kunizaki S, Shimaguchi M, et al. Superior mesenteric venous thrombosis after laparoscopic exploration for small bowel obstruction. Case Rep Surg. 2013;2013. https://doi.org/10.1155/2013/952383
6. Kaminsky M, Hochman D. Superior mesenteric venous thrombosis. CMAJ. 2011;183(6):693. https://doi.org/10.1503/cmaj.092134
7. Egwuonwu S. Acute superior mesenteric vein thrombosis in a patient with primary antiphospholipid syndrome: a case report and brief review of the literature. J Gastrointest Dig Syst. 2015;5:360. https://doi.org/10.4172/2161-069X.1000360
8. Warshauer DM, Lee JKT, Mauro MM, White GC. Superior mesenteric vein thrombosis with radiologically occult cause: a retrospective study of 43 cases. Am J Roentgenol. 2001;177(4):837-841. https://doi.org/10.2214/ajr.177.4.1770837
9. Efremidou EI, Kouklakis G, Tsirogianni O, Courcoutsakis N, Manolas KJ, Liratzopoulos N. Massive intestinal ischemia, a rare complication of oral contraceptive-induced mesenteric venous thrombosis: a case report and review of literature. Cases J. 2009;2:7416. https://doi.org/10.1186/1757-1626-2-7416
10. Koyama N. Superior mesenteric vein thrombosis associated with hormonal contraceptive use. Case Rep Gastroenterol. 2016;10(2):264-268. https://doi.org/10.1159/000446838
11. Gaspary MJ, Auten J, Durkovich D, Gable P. Superior mesenteric vein thrombosis mimicking acute appendicitis. West J Emerg Med. 2011;12(2):262-265. https://westjem.com/case-report/superior-mesenteric-vein-thrombosis-mimicking-acute-appendicitis.html
12. Pujahari AK. Challenges in the management of mesenteric vein thrombosis. J Mahatma Gandhi Inst Med Sci. 2015;20(2):163-166. https://doi.org/10.4103/0971-9903.164243
13. Kim H-K, Chun JM, Huh S. Anticoagulation and delayed bowel resection in the management of mesenteric venous thrombosis. World J Gastroenterol. 2013;19(30):5025-5028. https://doi.org/10.3748/wjg.v19.i30.5025